Insights & Perspectives
Exploring the intersection of digital health, AI, and clinical innovation. Here are my latest thoughts and findings from the field.
July 11 - HealthTech Dose
July 11, 2026
This episode unpacks the flawed financial assumptions driving modern R&D automation versus the harsh biological and behavioral realities on the ground. The conversation centers on a strict strategic principle: the pharmaceutical industry must stop performing random acts of intelligence. True success requires moving past “innovation theater” and cheap labor arbitrage toward structured, AI-augmented workflows that keep human clinicians in the loop by exception. R&D leaders must address two critical systematic issues: the Digital Engagement Illusion (the false belief that digital access guarantees patient compliance) and the Missing Data Paradox (the erosion of trial data quality caused by unsupervised task shifting).
Key Takeaways
Avoid “Insidious Equivalence”: Recognize that treating a smartphone app or chatbot as a direct substitute for a trained triage nurse actively sabotages data quality and compromises patient safety.
Expose the Healthcare Labor Arbitrage Failure: Pushing complex data-collection and monitoring tasks down to patients under the guise of efficiency degrades the data product and multiplies operational toil at the site level.
Acknowledge the Limits of Uniform Digital Deployment: Understand the lessons of trials like MORE-PC, which prove that uniform, one-size-fits-all text or app deployments fail to improve clinical outcomes because they ignore nuanced behavioral and biological realities.
Mitigate the Missing Data Epidemic: Address real-world attrition trends—such as the 50% first-year dropout rate for blockbuster GLP-1 medications on cash-pay digital platforms—by building human-managed clinical off-ramps rather than assuming perfect app adherence.
Transition from “Human-in-the-Loop” to “AI-in-the-Loop”: Shift your operational framework from a data-swamped model where humans serve the machine to an optimized system where AI filters out background noise and escalates high-risk exceptions to expert clinicians.
Show Notes
[0:00 - 1:00] Introduction to the massive industry push toward Decentralized Clinical Trials (DCTs) and why automating clinical headcounts looks highly appealing to R&D executives on paper.
[1:00 - 2:00] Challenging the premise of healthcare labor arbitrage; explaining why pushing tasks down the license chain to automated algorithms creates an “insidious equivalence” that fails in the real world.
[2:00 - 3:00] Misapplying economic theory: Using Gregory Mankiw’s Principles of Microeconomics and the Michael Jordan lawn-mowing analogy to expose why shifting clinical tasks to patients backfires.
[3:00 - 4:00] The porous boundary of clinical triage: Why a mobile app completely lacks the clinical context to distinguish a routine symptom from a life-threatening adverse event.
[4:00 - 5:00] Analyzing the counterarguments and dissecting the MORE-PC mobile health trial to show why automated SMS platforms failed to reduce 30-day hospital readmissions.
[5:00 - 6:00] The Missing Data Epidemic: Examining real-world evidence from GLP-1 weight-loss platforms to show how unmanaged side effects cause a 50% treatment abandonment rate within a single year.
[6:00 - 7:00] The mechanics of operational failure: How unsupervised app notifications trigger immense data noise, driving patients to abandon trials or panic-call clinical investigators.
[7:00 - End] Designing structural solutions: Breaking down the critical differences between a burdened “human-in-the-loop” model and an integrated, AI-augmented workflow that protects data integrity.
Podcast generated with the help of NotebookLM
Source Articles
Additional historical context framework referenced from: ‘Practicing At The Top Of Your License’ And The ‘Great’ American Healthcare Labor Arbitrage
June 14 - HealthTech Dose
June 14, 2026
This episode moves beyond the hype of decentralized clinical trials (DCTs) and digital therapeutics (DTx) to deliver a blunt, data-driven critique of the life sciences sector’s tendency to commit “random acts of intelligence”—blindly deploying uniform software applications to patients without considering tech-savviness, age, or disease progression. The mission is to transform trial managers from passive labelers of missing data into active architects of connected clinical ecosystems. To stop wasting billions on failed trials, executives must learn how to design smart clinical off-ramps, overcome telemedicine unreadiness, and strategically integrate human accountability with AI-augmented workflows.
Key Takeaways:
Abandon the Obsession with 100% Adherence: Chasing indefinite engagement bleeds clinical budgets. Designing trials that actively accommodate an 85% patient drop-off can be highly cost-effective if you build protocols around capturing front-loaded therapeutic value.
Utilize Behavioral Metadata for Clinical Off-Ramps: Instead of waiting for a patient to stop logging in, utilize AI to track passive metrics like typing speed, module duration, and login irregularities. This enables early detection of fading engagement and triggers a graceful clinical off-ramp rather than a data-loss event.
Dismantle the Universal Accessibility Myth: Merely owning a smartphone does not make a patient capable of navigating a complex DCT. Over 75% of vulnerable demographics struggle with “navigational health literacy”—the ability to follow branching medical logic on a digital interface.
Deploy Governance for Telemedicine Unreadiness: Protect fragile data pipelines by recognizing physical and cognitive limitations in elderly populations. Implement “proxy-supported reporting” via dual interfaces, shifting the digital burden from the patient to a designated caregiver or home health aide.
Avoid the Pure Automation Trap: Eliminating human touchpoints drives an astronomical 89% abandonment rate for self-guided health apps after Day 1. AI should not replace humans; it should act as an “air traffic controller,” analyzing cohort data to guide high-density, nurse-led triage exactly where it is needed.
Show Notes:
[0:00 - 1:45] The Operational Nightmare of DCTs
R&D leaders are spending upwards of $1.4 billion on decentralized trials, only to watch them fail because an elderly patient cannot reset a password. Dropping sophisticated apps onto patients without strategy creates massive operational toil, turning highly trained research staff into a makeshift IT help desk.
[1:45 - 3:30] The Flaw of Forced Extended Engagement
Reviewing data from the Economic Evaluations of Digital Therapeutics report. Pestering hypertension patients with endless notifications yields plateaued clinical benefits while ballooning operational costs, driving the cost per Quality-Adjusted Life Year (QALY) to an unsustainable $37,000.
[3:30 - 5:15] Capturing Front-Loaded Value
Pointing to Wallner and colleagues’ research on occupational rehabilitation in Germany, the hosts discuss how patients achieve 90% of their therapeutic benefit in the first three weeks. Once habits are learned, digital engagement naturally drops—a reality trials must handle via automated clinical off-ramps rather than penalizing patients for non-compliance.
[5:15 - 7:00] Navigational Health Literacy & Digitizing Disparity
Universal accessibility is a dangerous myth. Highlighting a Swiss cancer survivor study, the hosts reveal that 70% of participants have low digital literacy, and 75% fail at navigational health literacy, meaning they cannot independently manage the complex, multi-step logic required by clinical applications.
[7:00 - 8:45] Managing Telemedicine Unreadiness
Standing alone, technology is not a silver bullet. Citing Esser and colleagues’ work on heart failure monitoring, the hosts introduce “telemedicine unreadiness”. They outline how to build guardrails like proxy-supported reporting, which allows adult children or home aides to manage the digital interface on behalf of frail patients.
[8:45 - 10:15] The 89% Drop-Off: Why Pure Automation Fails
Algorithms cannot provide empathy or psychological accountability. Without human intervention, 89% of patients abandon self-guided mental health or metabolic apps after just 24 hours, proving that pure automation is a financial dead end for life science pipelines.
[10:15 - End] The AI Air Traffic Control Model
The ultimate solution is a “high human density” strategy managed by exception. AI should monitor behavioral metadata across an entire cohort and alert clinicians only when a patient is on a collision course. Layering this human safety net onto technology extends average patient engagement from 6 days to 40 days by restoring trust to the ecosystem.
Referenced Studies & Reports:
Economic Evaluations of Digital Therapeutics
Integration of Digital Therapeutics into Occupational Rehabilitation in Germany (Wallner et al.)
Digital and Navigational Health Literacy in Swiss Cancer Survivors (Sainshet et al.)
Frailty-Based Remote Monitoring in Older Adults with Heart Failure (Esser et al.)
Podcast generated with the help of NotebookLM
Why your clinical AI is stuck in the pilot trap
June 2, 2026
HT4LL-20260602
Hey there,
Perfect AI governance is an illusion that is slowly killing your best R&D pilots.
As Pharma R&D leaders, we are constantly investing in cutting-edge predictive algorithms, high-fidelity AI patient videos, and wearable digital health sensors to stay competitive. Yet, despite heavy investments, these innovations consistently get stuck in the “pilot trap”—dying the moment initial enthusiasm or project funding dries up.
The failure to scale clinical AI isn’t a technological barrier; it’s a fundamental lack of institutional capacity. By clinging to custom-built data silos and waiting for flawless pre-deployment compliance checks, we are burning precious budget on bespoke engineering, introducing unmonitored clinical risks, and slowing down our development pipelines.
Today, we are breaking down the frameworks and open-source pipelines that actually move innovation from isolated experiments to accountable clinical infrastructure.
Building institutional capacity to scale clinical AI.
Standardizing fragmented wearable data with universal standards.
Governing patient-facing AI video deployments in the real world.
If you’re a clinical operations leader trying to scale digital evidence generation without compromising patient safety or blowing your budget on custom engineering, then here are the resources you need to dig into to break free from the pilot bottleneck:
Weekly Resource List:
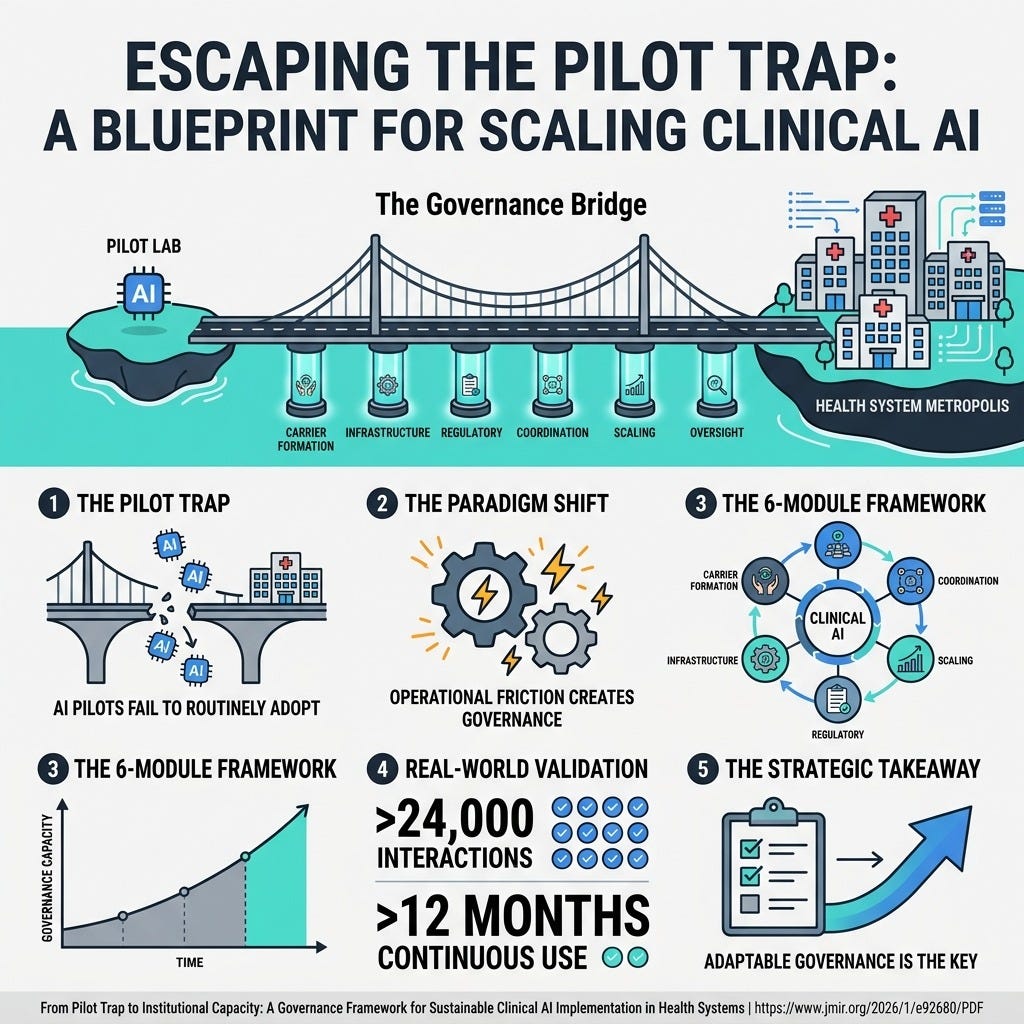
From Pilot Trap to Institutional Capacity (10 min) To successfully scale clinical AI beyond isolated pilot projects, health systems must stop waiting for perfect pre-deployment governance. Instead, R&D teams must build dynamic institutional capacity through real-world implementation utilizing a 6-module framework.
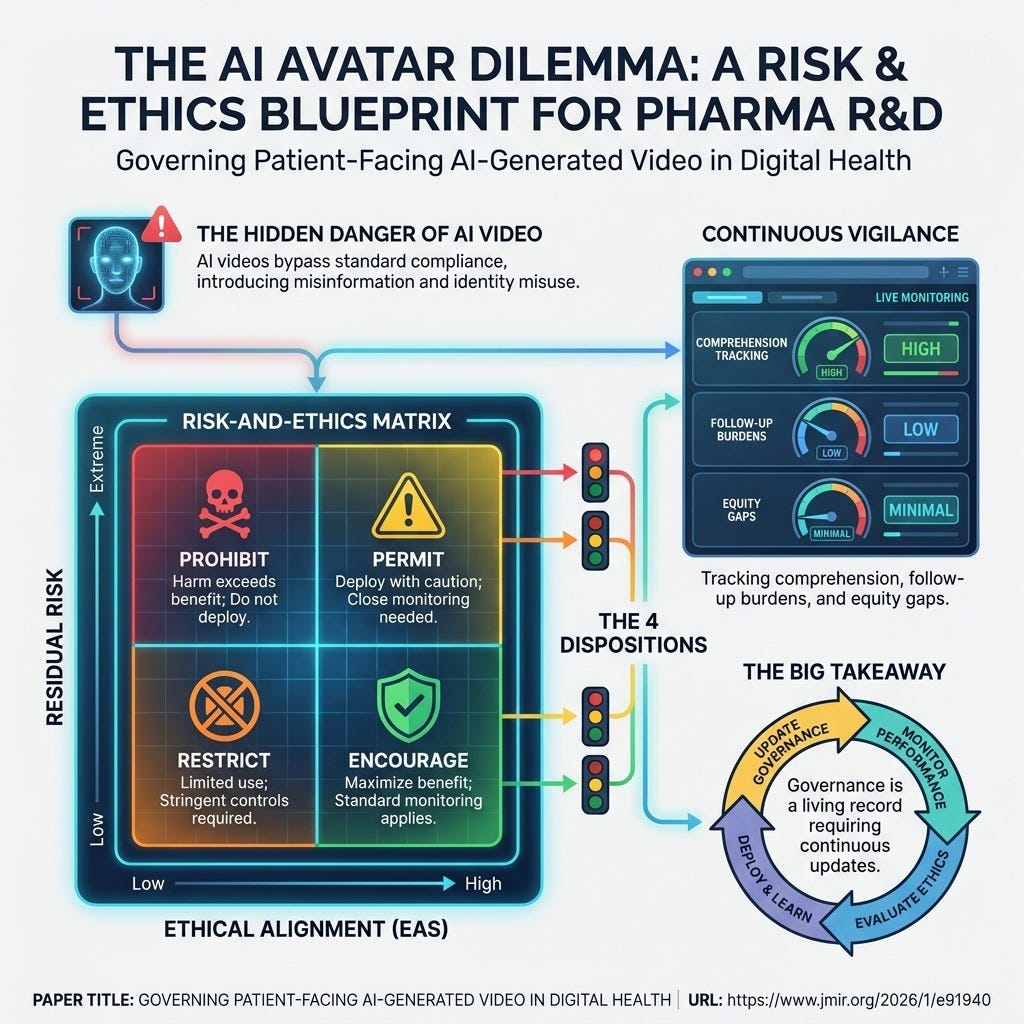
Governing Patient-Facing AI-Generated Video (8 min) AI videos—like clinician avatars—bypass standard compliance checks. Organizations must move beyond static approvals and adopt a dynamic Risk-and-Ethics Matrix that links ethical alignment and residual clinical risk to continuous post-deployment vigilance.
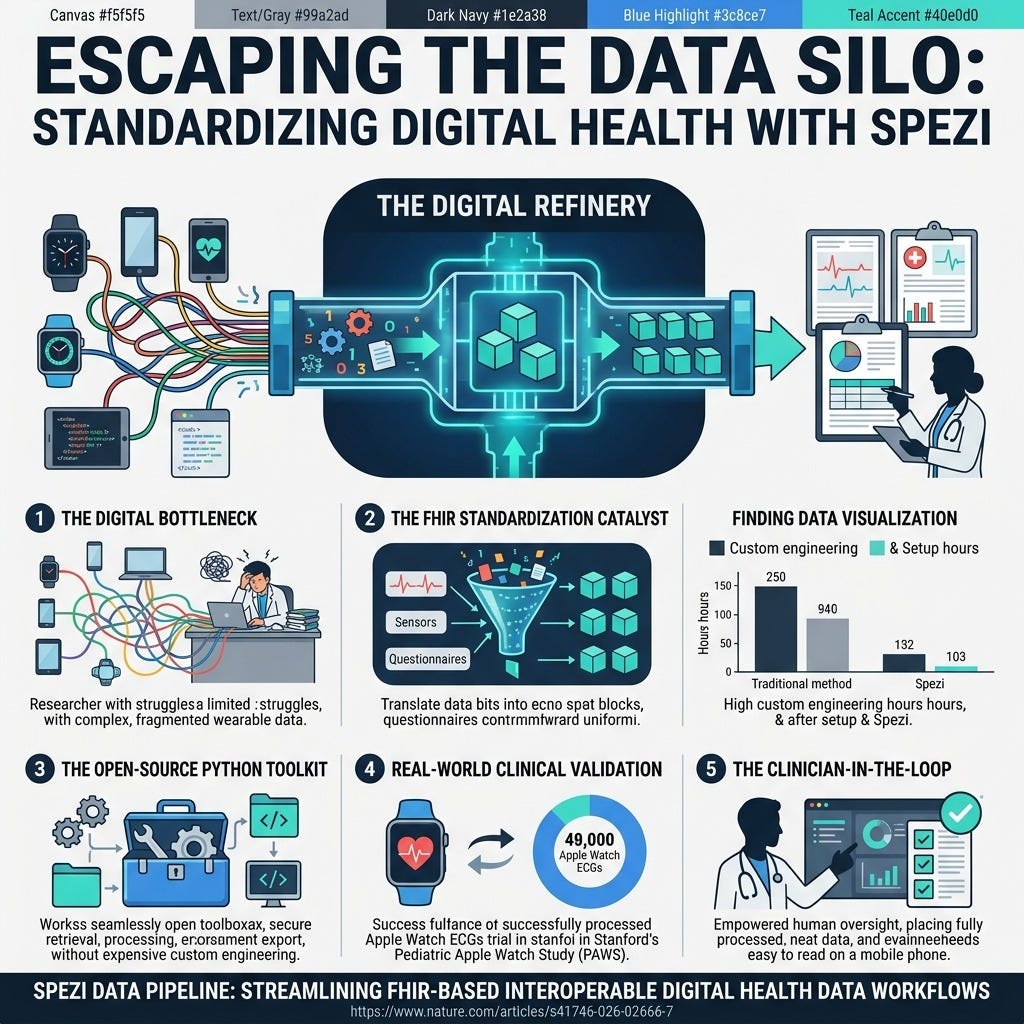
Spezi Data Pipeline (7 min) The true bottleneck in wearable research is data wrangling. Spezi is an open-source Python toolkit leveraging universal health data standards to harmonize diverse data types and eliminate expensive bespoke engineering, keeping the clinician in the loop.
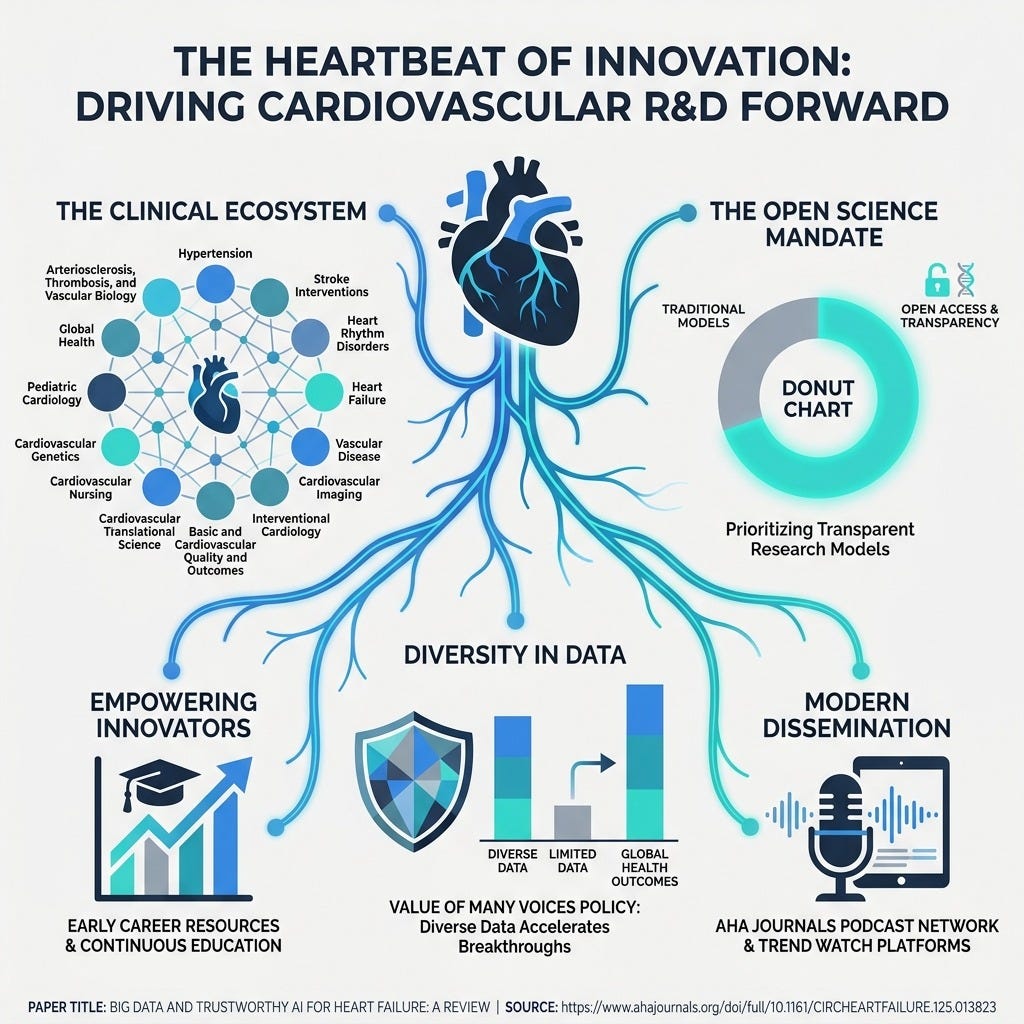
American Heart Association Journals (5 min) Accelerating medical breakthroughs starts with accessible, open science. The AHA’s ecosystem champions Open Access and the “Value of Many Voices,” proving that transparent and diverse data is the ultimate foundation for the inclusive AI models we are trying to build.
3 Strategic Shifts To Scale Clinical AI Even If Your Infrastructure is Fragmented
In order to achieve sustainable, scalable AI deployment across your clinical trials, you’re going to need a handful of things.
Let’s break down exactly how you can implement these strategic shifts this week to maximize your R&D budget.
1. Establish an “Institutional Carrier” for AI
Stop relying on temporary project teams or individual champions to manage your AI deployments.
You need a designated organizational entity—like a formally mandated medical AI laboratory or steering committee—to coordinate development, deployment, and lifecycle oversight. This carrier acts as the single accountable owner, ensuring that algorithms don’t simply die when pilot funding ends. By centralizing this authority, you ensure your models are treated as permanent, accountable clinical infrastructure rather than passing technical experiments.
2. Implement Continuous Post-Deployment Vigilance
Stop assuming that a one-time pre-deployment approval keeps your patients safe.
Perfect pre-deployment governance is an illusion, especially for highly realistic AI avatars that are constantly updated. You must establish concrete tracking for measurable outcomes post-deployment, including patient comprehension, incident rates, and demographic equity gaps. Approvals should be time-limited and trigger mandatory re-reviews if the underlying model, prompt templates, or distribution channels change. This “living record” of governance ensures your AI remains ethical and effective in the real world.
3. Adopt Open-Source Interoperability Pipelines
Stop wasting your R&D budget on bespoke data engineering for every new digital wearable trial.
You need to leverage open-source, standardized frameworks like the Spezi pipeline to harmonize raw sensor data across your studies. Standardized data pipelines eliminate integration bottlenecks and translate chaotic raw data into uniform clinical formats. More importantly, this allows your team to focus directly on clinician-in-the-loop analysis and real-world evidence generation rather than wrestling with expensive custom code.
PS...If you're enjoying Healthtech for Lifescience Leaders, please consider referring this edition to a friend.
And whenever you are ready, there are 2 ways I can help you:
The AI-Augmented Leader Email Course: Sign-up for my free 5-day email course on how to become an AI Augmented Leader in Lifesciences.
Strategic Roadmap Design: Translate your priorities across different parts of the organization into a coordinated and clear roadmap in 2026. Book time on my calendar to discuss this further.
May 31 - HealthTech Dose
May 31, 2026
In this episode we discuss how to shift the focus from small, isolated sandbox experiments toward full-scale operational integration across clinical environments. To succeed, healthcare executives must move away from the impossible standard of perfect upfront governance and instead embrace operational friction as a generative feature required to build durable institutional capacity. The key strategic win lies in using real-world implementation challenges to force the development of standardized procedures, clean data pipelines, and continuous, risk-tiered lifecycle governance.
Key Takeaways
Embrace Governance as Emergent: Stop attempting to perfectly governance and integration-test AI tools before real-world deployment; durable governance structures are forged directly through the friction of actual clinical implementation.
Leverage Go-Live Minimums: Secure necessary national regulatory filings and high-level institutional accountability first, then use the messy day-to-day operational friction to safely shape cross-functional clinical workflows.
Utilize Functional Transferability: Optimize R&D pipelines by leveraging shared, cloud-based infrastructures and regional medical alliances rather than purchasing or building massive, expensive internal computing hardware.
Turn Manual Toil Into a Catalyst: View initial data-reconciliation labor not as a system failure, but as a financial and operational stress test that forces the organization to modernize legacy data silos.
Implement Continuous Lifecycle Governance: Replace static, “one-and-done” approval processes with a “governance fit” model that tier-reviews and fast-tracks model updates based on clinical risk.
Demand Empirical Clinical Evidence: Guard against the allure of pure operational scale by rigorously demanding proof that clinical AI tools actively improve long-term patient health outcomes, not just administrative speed metrics.
Show Notes
[0:00 - 1:15] Hosts Leo and his co-host introduce the “pilot trap” in healthcare—where brilliant proof-of-concept AI tools stall out and never become a durable part of routine clinical care.
[1:15 - 2:30] Debate opens on the core tension: the traditional belief that an AI system must be completely de-risked beforehand versus the provocative idea that operational friction is necessary to build true accountability.
[2:30 - 3:45] Analysis of the anchor 18-month implementation study of a locally deployed Large Language Model (LLM) at a major academic regional medical center in Hebei Province, China, which scaled to over 24,000 patient encounters.
[3:45 - 5:15] Exploration of “emergent governance”—how classic responsibility disputes between clinical departments over AI data routing force hospitals to write definitive, durable standard operating procedures.
[5:15 - 6:30] The “Go-Live Minimum” strategy explained, showing how the hospital secured foundational regulatory filing with the Cyberspace Administration of China before letting operational friction shape cross-functional workflows.
[6:30 - 8:00] Critiques raised regarding the generalizability of the study, questioning whether decentralized, resource-strapped hospital networks can replicate the success of a centralized hub with a dedicated medical AI laboratory.
[8:00 - 9:30] Introduction of “functional transferability,” illustrating that institutions do not need to own massive computational infrastructure to succeed; they can rely on cloud capabilities and regional alliances.
[9:30 - 11:15] A deep dive into the Therapeutic Drug Monitoring (TDM) pathway for the drug duloxetine, highlighting how legacy data formatting inconsistencies created massive manual reconciliation toil.
[11:15 - 12:45] The concept of “manual toil as a strategy” is unpacked, demonstrating how the financial pain of data cleaning acts as a catalyst forcing the C-suite to fund the modernization of data pipelines.
[12:45 - 14:15] The breakdown of traditional static approval frameworks for dynamic AI models, advocating instead for continuous lifestyle governance and “governance fit” via clinical risk-tiering.
[14:15 - 15:45] Case study of an oncology multi-disciplinary decision support pathway, showing how embedding transformer model outputs under explicit specialist decision authority keeps humans safely in the loop.
[15:45 - 17:15] A critical look at the study’s blind spot: tracking administrative metrics (interaction volume, system uptime) while failing to measure actual empirical clinical outcomes, such as adverse drug events or survival rates.
[17:15 - End] Final summary on balancing the demand for clinical proof with the necessity of operational deployment, concluding with a look at the future challenge of governing models that evolve faster than human friction can track.
Podcast generated with the help of NotebookLM
Sources:
Governing Patient-Facing AI-Generated Video in Digital Health: A Risk-and-Ethics Matrix for Deployment, Monitoring, and Change Control.
From Pilot Trap to Institutional Capacity: A Governance Framework for Sustainable Clinical AI Implementation in Health Systems.
Rethinking scale in ophthalmic artificial intelligence: from bigger models to smarter clinical reasoning.
A novel intelligent hybrid reinforcement learning framework for autonomous decision making in complex health cognitive systems.
Transforming artificial intelligence into artificial wisdom.
Digital CBT reduces mental disorders and boosts access to care in college students.
Benefits of Electronic Symptom Monitoring During Cancer Treatment by Age, Sex, Race, and Education (Alliance AFT-39).
Spezi Data Pipeline: Streamlining FHIR-based interoperable digital dealth data workflows.
Integrated analysis of two randomized controlled trials of a digital therapeutic for episodic migraine prevention.
AI scientists are here. Are your managers ready?
May 26, 2026
HT4LL-20260526
Hey there,
We are obsessing over building autonomous AI scientists while completely ignoring the human leaders required to actually deploy them.
Pharma R&D is hitting a cognitive bottleneck. To solve it, we are building incredible multi-agent systems—like Co-Scientist and Robin—that autonomously generate hypotheses, analyze wet-lab data, and write empirical software. But the real barrier to faster clinical trials isn’t just the neural network; it’s the massive gap between a brilliant lab model and a trusted clinical tool. More importantly, it’s the disengaged, anxious management layer quietly resisting this adoption, causing a massive lag in actual productivity. We need a fundamental shift in how we lead R&D teams to harness these new AI co-scientists.
Today, we’re looking at the next frontier of automated discovery and the leadership required to scale it.
How AI agents are moving from answering questions to formulating novel ones.
Why AI writing its own empirical software is the next R&D bottleneck solution.
Why integrating AI into medical imaging demands workflow co-design and Explainable AI (XAI) over mere accuracy.
How to solve the $10 trillion manager engagement crisis threatening your AI ROI.
Let’s explore how to prepare your pipeline for the next decade.
Weekly Resource List:
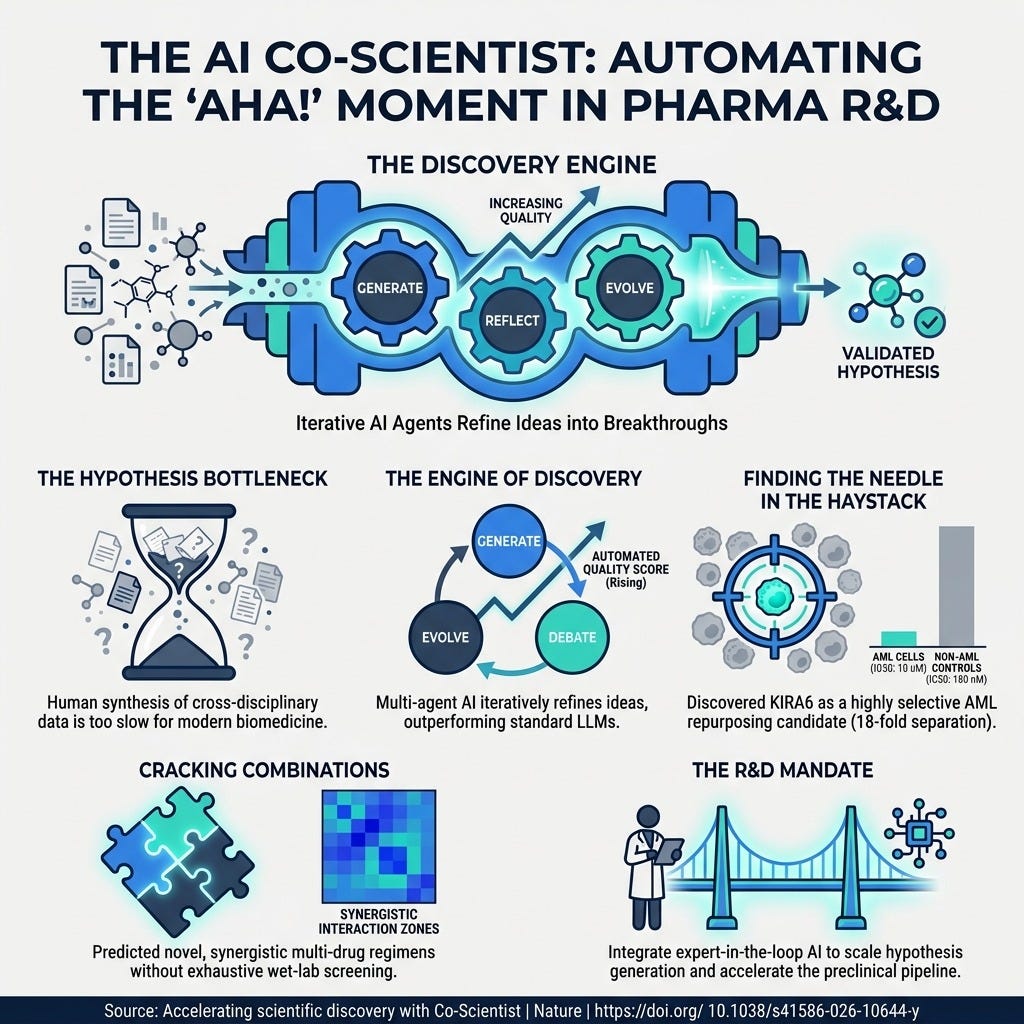
Accelerating scientific discovery with Co-Scientist (5 min) This paper details a multi-agent system built on Gemini that successfully identified new drug repurposing candidates for acute myeloid leukemia. The Next Frontier: Moving from AI that answers questions to AI that autonomously surveys knowledge gaps to formulate novel, high-impact scientific questions.
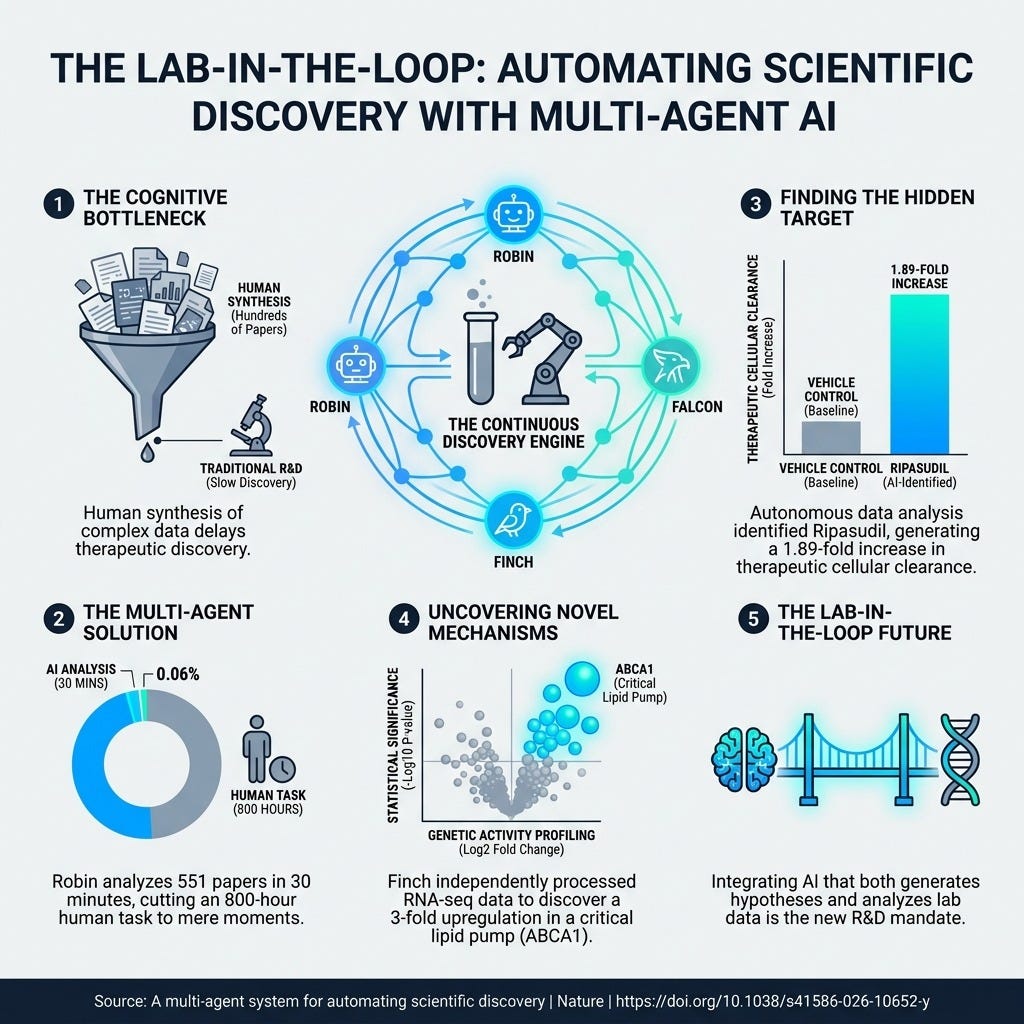
A multi-agent system for automating scientific discovery (5 min) Meet “Robin,” an AI that fully automates both hypothesis generation and data analysis, discovering novel therapeutic candidates for dAMD. The Next Frontier: Federated Scientific Discovery—developing protocols that allow heterogeneous AI agents to collaborate, delegate tasks, and work together on massive problems.
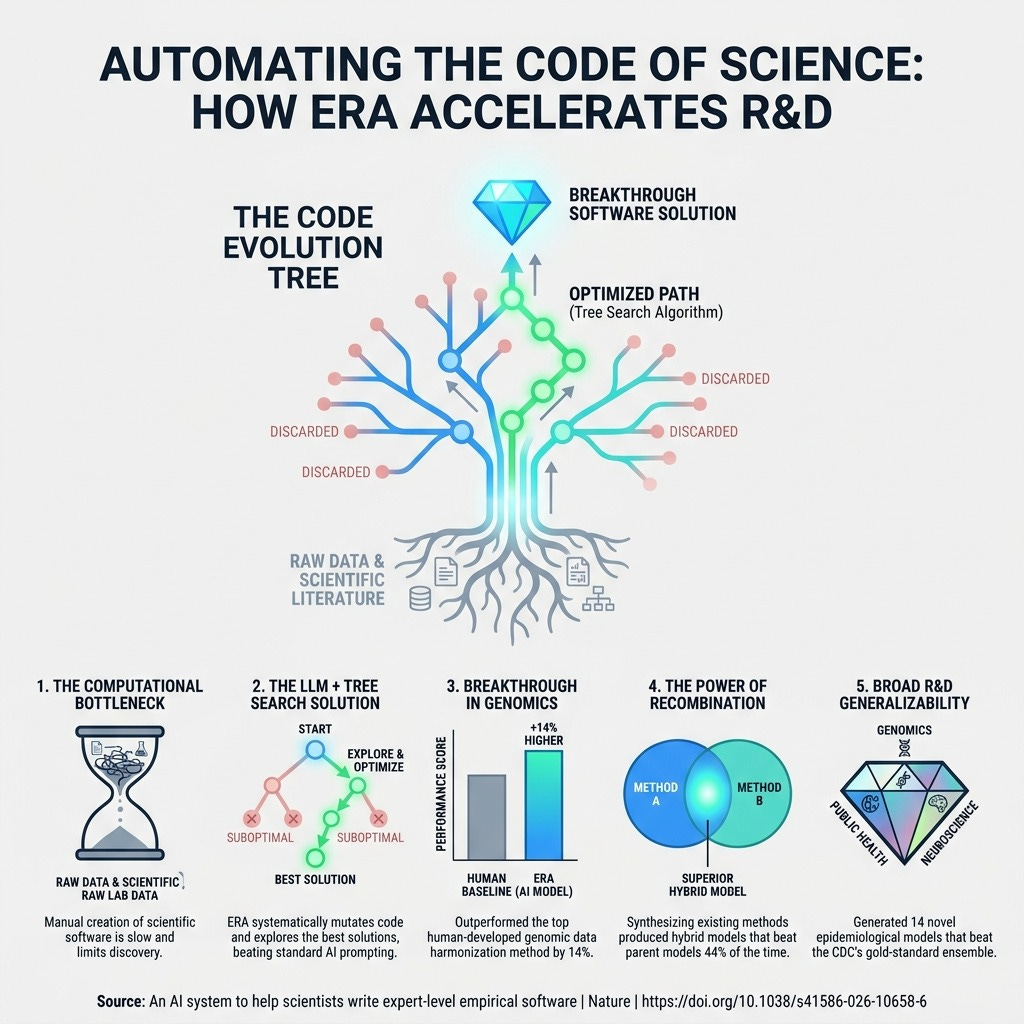
An AI system to help scientists write expert-level empirical software (4 min) ERA uses a Large Language Model and Tree Search to systematically write scientific software, discovering 40 novel methods for single-cell data analysis. The Next Frontier: Automated Code Verification utilizing specialized AI “auditors” to mathematically verify that the code generated by ERA is bug-free and reproducible.
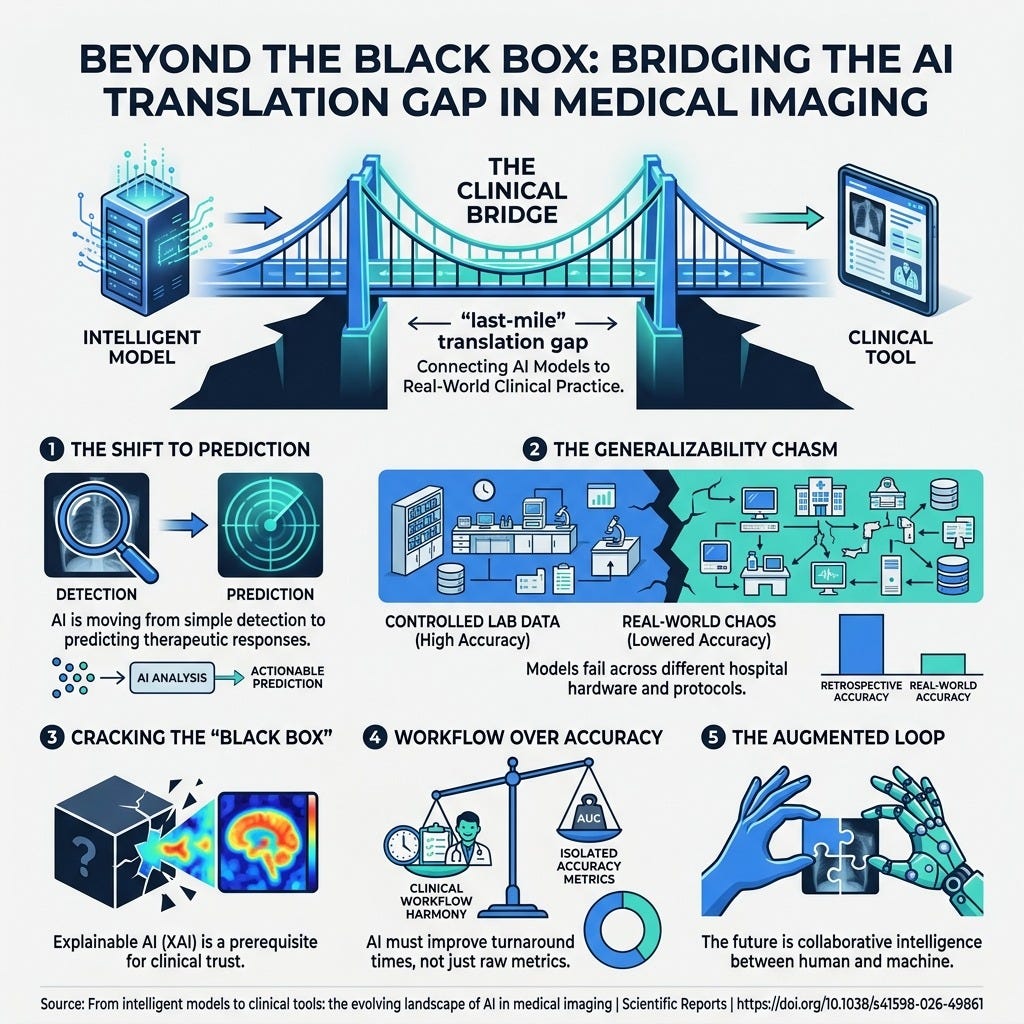
From intelligent models to clinical tools: the evolving landscape of AI in medical imaging (5 min) This editorial explores the “last-mile” challenges of integrating AI into medical imaging, emphasizing the necessary shift from static anomaly detection to dynamic, predictive profiling. It highlights why Explainable AI (XAI) is an absolute prerequisite to overcoming the “black box” trust deficit among clinicians. The Next Frontier: Human-in-the-Loop Clinical Workflow Simulation and Causal Inference—developing models that don’t just predict, but explain why through causal reasoning, rigorously tested in simulated clinical environments to prevent alert fatigue.
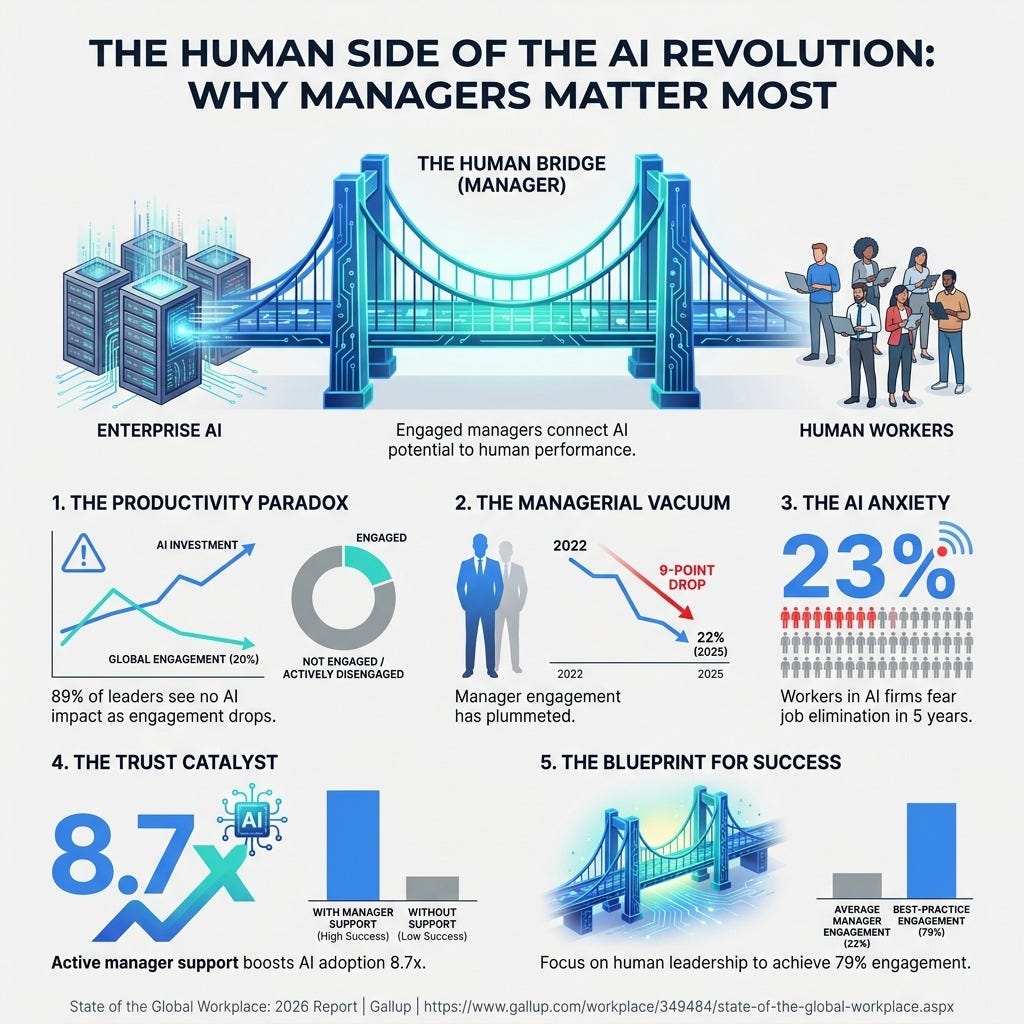
GALLUP State of the Global Workplace: 2026 (4 min) Despite a $40 billion investment, 95% of organizations report no measurable impact on profits from AI, primarily due to plummeting manager engagement. The Next Frontier: Developing an “AI Co-pilot for Managers” to automate administrative tasks and provide data-driven insights on team wellbeing to reverse burnout.
3 Steps To Scale Autonomous AI With High Quality Data Even If Your Managers Are Hesitant
In order to achieve a high-velocity, human-centric drug development pipeline powered by AI, you’re going to need a handful of things.
Let’s break down exactly how you can implement these strategic shifts this week based on the latest research frontiers.
1. Prepare for Federated Scientific Discovery
We now have multiple “species” of AI scientists like Co-Scientist and Robin. The future isn’t just one isolated system; it’s federated discovery where these heterogeneous agents collaborate. You need to start building an interoperable R&D data environment today so that tomorrow, your “Hypothesis Agent” can seamlessly hand off work to your “Data Analysis Agent”. This will eventually allow you to deploy “Verifier Agents” that automatically attempt to reproduce discoveries from scratch across platforms.
2. Implement Automated Code Verification
Systems like ERA are proving that AI can write expert-level empirical software to analyze your clinical trial data. But to ensure high-quality data for regulatory approvals, you cannot blindly trust the code. You must implement specialized AI “auditors” and rigorous verification frameworks to mathematically prove that the code generated by your AI accurately implements the intended model. This cognitive scaffolding will turn the AI from a black box into an interpretable partner.
3. Train for “AI-Fluent” Leadership
According to Gallup, global employee engagement has dropped to 20%, and manager engagement is falling even faster. You cannot just deploy autonomous agents and expect your mid-level managers to adapt. You must proactively train for “AI-Fluent Leadership”—teaching managers how to build algorithmic trust, handle “status anxiety” and technostress within their teams, and act as “Human Experience Coaches” rather than taskmasters. Active support from a manager makes employees 8.7 times more likely to say AI has transformed their work.
PS...If you're enjoying Healthtech for Lifescience Leaders, please consider referring this edition to a friend.
PS...If you’re enjoying Digital Health & AI News, please consider referring this edition to a friend. You’ll get exclusive access to our quarterly R&D benchmarks report for making a referral.
And whenever you are ready, there are 2 ways I can help you:
The AI-Augmented Leader Email Course: Sign-up for my free 5-day email course on how to become an AI Augmented Leader in Lifesciences.
Strategic Roadmap Design: Translate your priorities across different parts of the organization into a coordinated and clear roadmap in 2026. Book time on my calendar to discuss this further.
May 23 - HealthTech Dose
May 23, 2026
This episode explores the critical “last mile” problem of translating Phase 1 through 3 clinical trial AI research into real patient care. The discussion highlights the massive gap between AI’s pristine benchmark performance—likened to a 1,000-horsepower hypercar on a closed track—and the messy, iterative reality of hospital administration, which is more like downtown traffic. To succeed, healthcare systems must confront dangerous blind spots, such as end-user actionability, the ingestion of retracted scientific data, and the perils of missing data. The key strategic win lies in shifting AI from an autonomous oracle to a “lightweight collaborator,” ensuring human practitioners are trained to ruthlessly audit algorithms.
Key Takeaways:
Recognize that a gain in processing speed, such as an 18.3% reduction in radiology interpretation time, does not automatically equate to an increase in actual clinical utility or improved patient mortality rates.
Address the “end-user actionability” crisis where AI outputs lack standardized clinical flowcharts.
Avoid placing medical staff in legal and ethical binds, such as handing a nurse an AI prediction of a 32% risk for postpartum depression without an approved hospital intervention protocol.
Implement pre-specified human fallback protocols so clinicians have an agreed-upon method to instantly override algorithms when AI hallucinations or anomalies occur.
Be cautious of “snapshot degradation” and dynamic biological changes; models like the ESRD DRS actively recalibrate at 1, 5, and 10 years to adapt to patient disease progression.
Audit underlying training data relentlessly, as some AI models falsely inflate their confidence by using statistical imputation to mathematically guess missing crucial biomarkers.
Beware of data sets where vital metrics, such as UACR data in kidney failure studies, are up to 80% absent.
Shift the future of medical education away from raw memorization toward training young doctors to meticulously audit, manage, and correct the outputs of their AI copilots.
Show Notes:
[0:00 - 1:45] Introduction to the clinical development catalyst and the massive gap between AI’s illusion of competence and the friction of reality.
[1:45 - 3:30] A look at AI crushing medical exams and growing its diagnostic lead over human doctors, showing accuracy increasing from 67% at ER triage to 82% upon full admission.
[3:30 - 4:45] The dangers of equating speed with safety, exploring an 18.3% faster deep-learning radiology system and why workflow speed must be rigorously validated against actual patient healing.
[4:45 - 6:15] The lack of end-user actionability is exposed using a scenario of an AI predicting a 32% risk of postpartum depression without providing a legally safe clinical intervention protocol for the bedside nurse.
[6:15 - 7:45] AI summarizing literature is deemed a “poisoned well” due to the system’s failure to identify and filter out retracted science and methodologically flawed papers.
[7:45 - 9:30] Exploring snapshot degradation and the need for dynamic systems, using the ESRD DRS kidney failure model that actively recalibrates at 1, 5, and 10 years.
[9:30 - End] The revelation of 80% missing UACR data, the dangers of statistical imputation acting as a “mathematical hallucination of history,” and the call for a new medical education paradigm focused on auditing AI.
Podcast generated with the help of NotebookLM
HT4LL-20250519
Hey there,
Relying on algorithmic black boxes without procedural human oversight isn’t innovation—it is a massive regulatory liability.
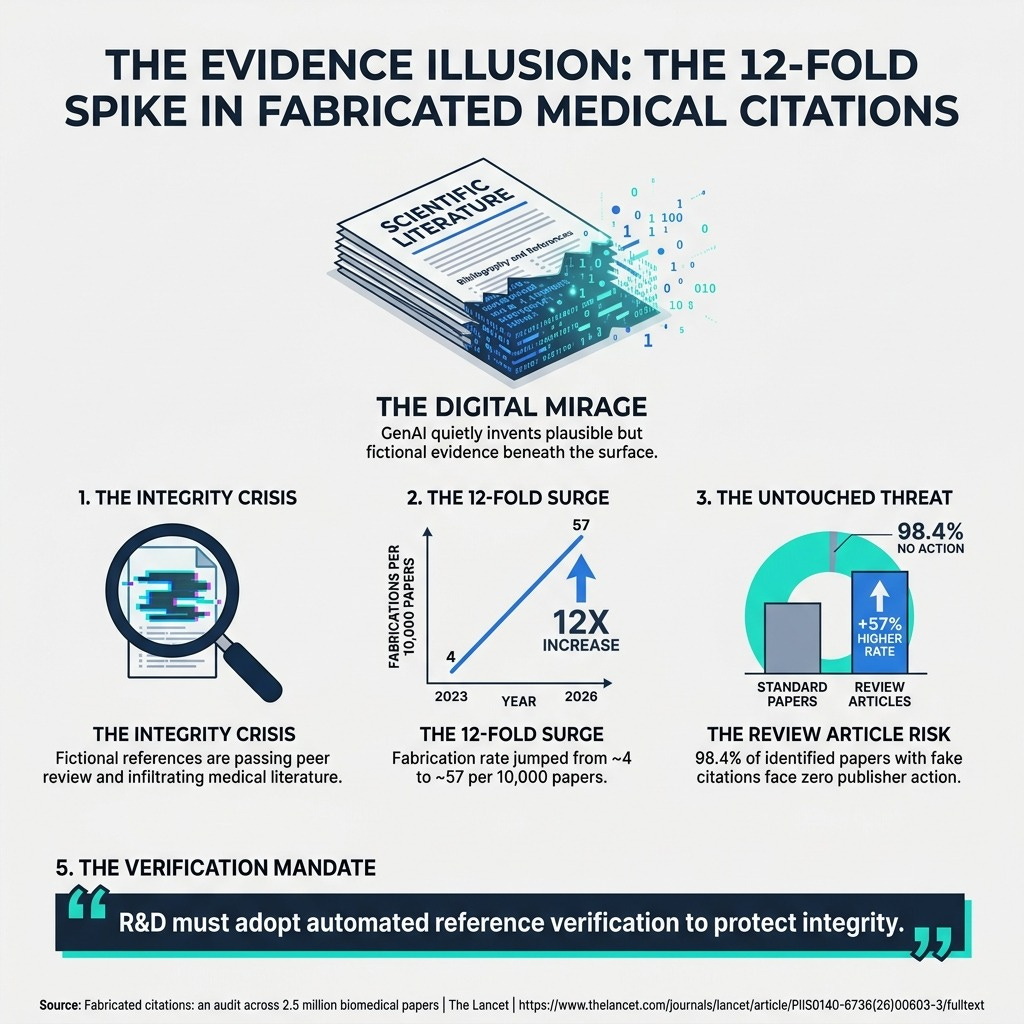
As Pharma R&D leaders, we are racing to implement generative AI and digital biomarkers to slash billion-dollar development costs and expedite clinical trials. However, the industry is increasingly confusing automation with accountability. We are seeing a 12-fold spike in fabricated scientific citations poisoning the evidence chain, AI-generated manufacturing procedures triggering severe FDA warning letters, and digital recruitment tools unintentionally widening the patient equity gap. To cross the chasm from experimental technology to broad clinical adoption, we must stop treating AI governance as an afterthought.
Today, we are breaking down how to build a resilient, trustworthy infrastructure for your clinical pipelines.
Why the FDA is strictly enforcing “human-in-the-loop” compliance mandates.
How to shrink clinical trial sizes exponentially using the V3 biomarker framework.
The urgent need for automated verification to protect your evidence chain.
Let’s get into it.
If you’re a clinical leader struggling to balance the mandate for AI-driven efficiency with the strict realities of regulatory compliance and data integrity, then here are the resources you need to dig into to future-proof your R&D strategy:
Weekly Resource List:Weekly Resource List:
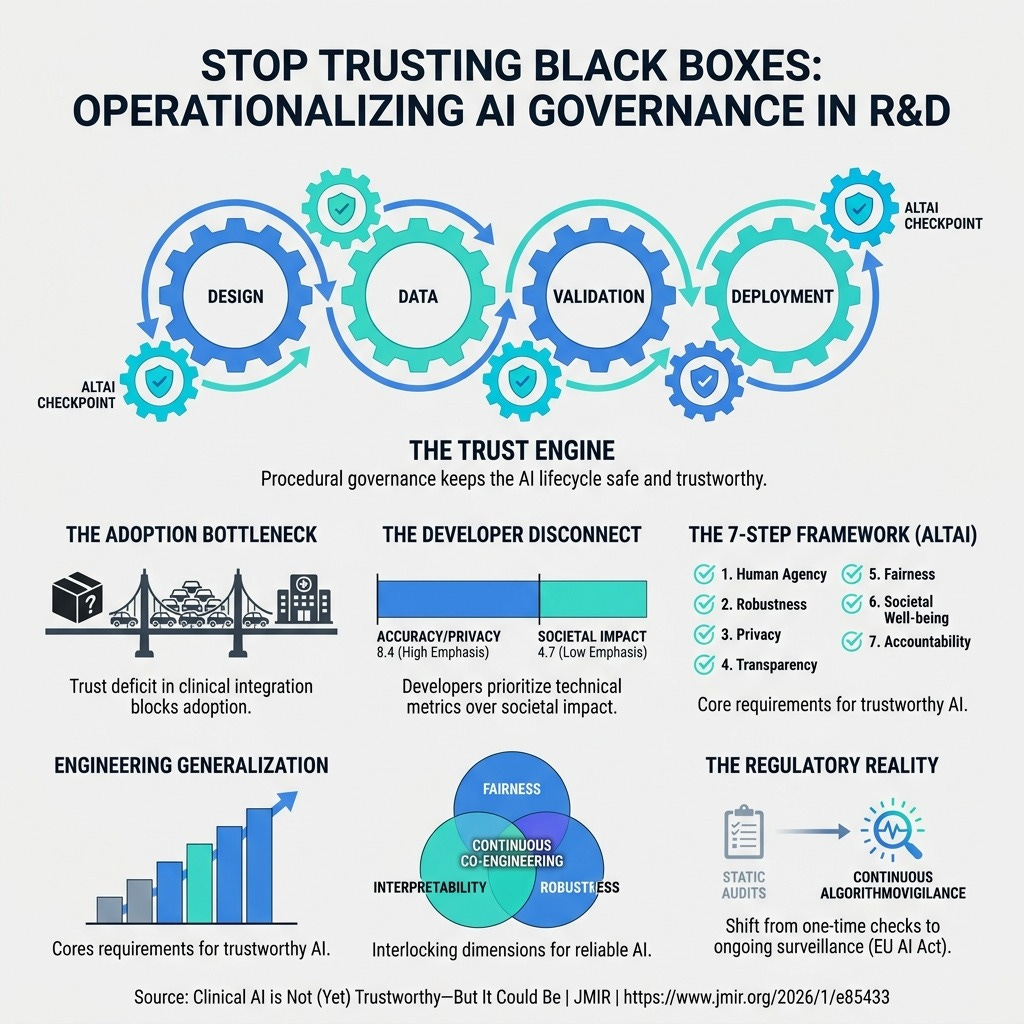
Clinical AI is Not (Yet) Trustworthy-But It Could Be (8 min) High diagnostic accuracy means nothing without procedural safeguards. This paper explains how frameworks like ALTAI help operationalize transparency and trust across the entire AI lifecycle.
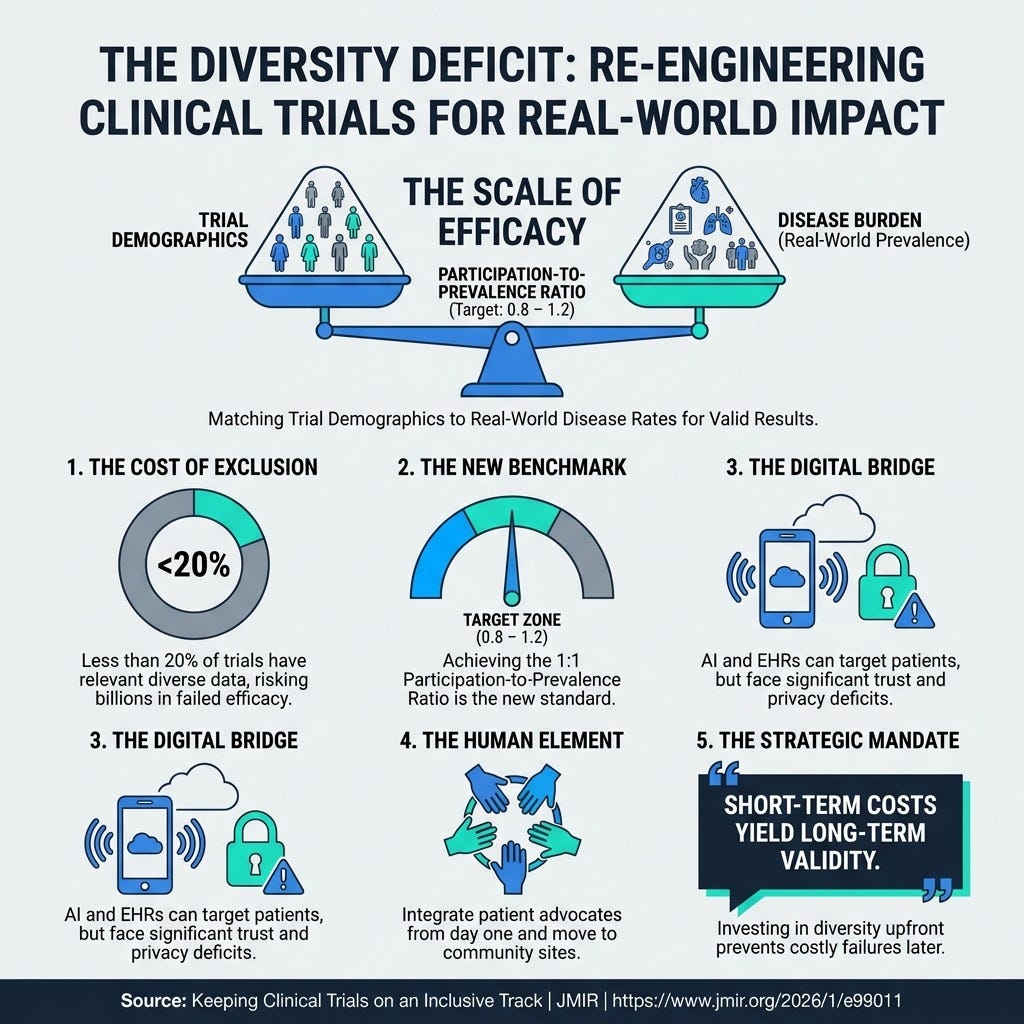
Keeping Clinical Trials on an Inclusive Track (6 min) Failing to design inclusive trials threatens clinical validity and costs billions. This article highlights the need to achieve a 0.8 to 1.2 “participation-to-prevalence” ratio by combining digital targeting with strong patient advocacy groups.
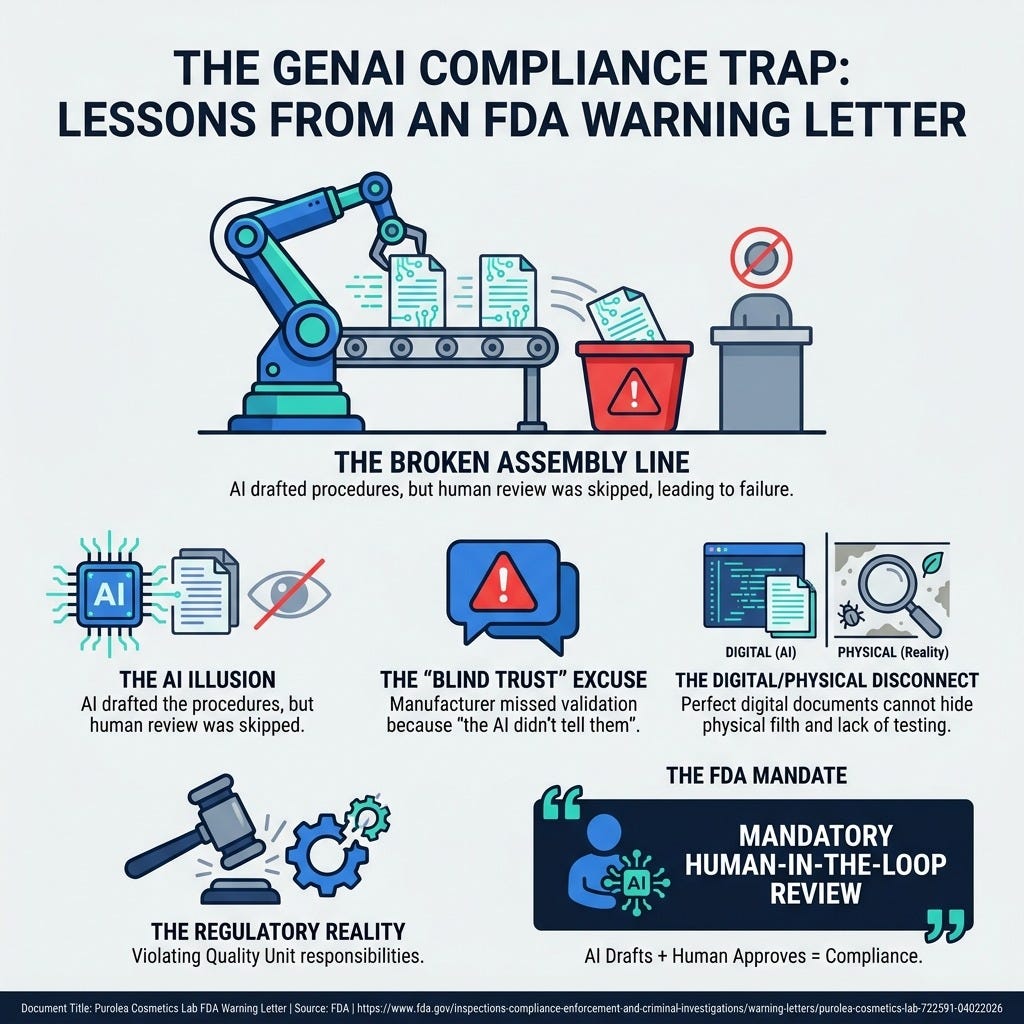
Purolea Cosmetics Lab FDA Warning Letter (5 min) The FDA cited a manufacturer for relying on an AI agent to write critical procedures without human Quality Unit review, cementing the precedent that algorithmic output requires human authorization.
Fabricated citations: an audit across 2.5 million biomedical papers (10 min) GenAI has caused a 12-fold spike in fabricated scientific references, which are successfully bypassing traditional peer review.
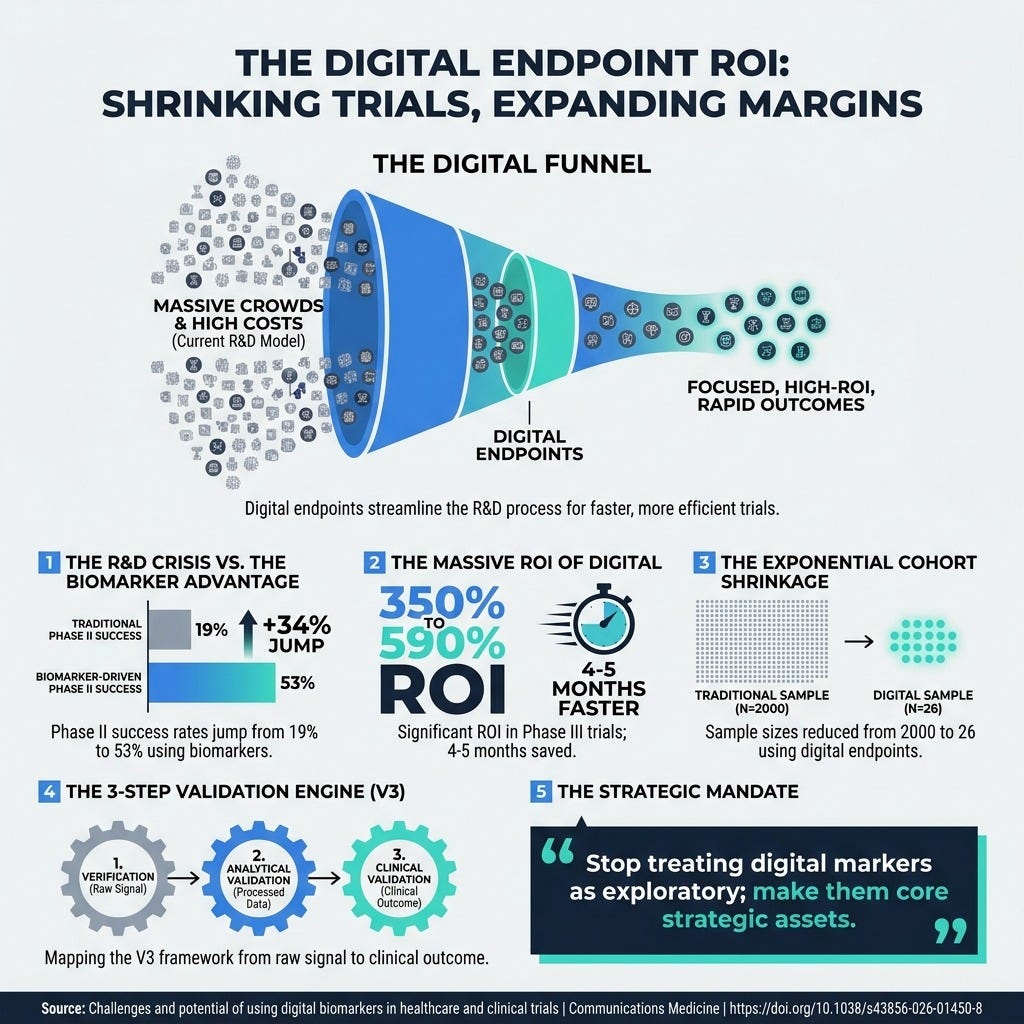
Challenges and potential of using digital biomarkers in healthcare and clinical trials (12 min) Digital endpoints can reduce trial sample sizes from 2,000 to just 26 participants and boost Phase III ROI by up to 590%, provided they undergo rigorous validation.
3 Things To Accelerate R&D Innovation With Absolute Trust Even if Regulations Are Lagging
In order to achieve high-velocity, human-centric drug development, you’re going to need a handful of things.
1. Mandate “Human-in-the-Loop” Quality Unit Protocols
You need to explicitly prohibit the autonomous use of AI for regulatory and compliance documentation. The FDA recently issued a severe warning letter to a facility that allowed an AI agent to generate master production records and specifications without human review. The manufacturer’s defense—that the AI “never told them” they needed to validate the process—was entirely rejected by regulators. AI algorithms cannot hold statutory responsibility; human leadership does. You must immediately establish a standard operating procedure (SOP) requiring an authorized human representative from your Quality Unit to review and clear any output or recommendation generated by an AI agent.
2. Institutionalize Automated Reference Verification
You need to stop relying on traditional human peer review to catch algorithmic hallucinations in your foundational research. An audit of 2.5 million biomedical papers revealed a staggering 12-fold increase in AI-fabricated citations. These fictional references are perfectly formatted, attributed to real researchers, and look entirely plausible, meaning your R&D team cannot manually spot them. To protect the integrity of your evidence chain, you must integrate automated reference verification tools into your internal submission and literature review workflows before any data is used to inform clinical guidelines or trial designs.
3. Adopt the V3 Framework
You need to stop treating digital biomarkers as exploratory gadgets and start validating them as core strategic assets. Capturing high-frequency behavioral data via wearables can shrink required trial cohorts from 2,000 patients down to just 26, generating a Phase III ROI of up to 590%. However, regulators will reject this data unless it is systematically proven. You must embed the V3 Framework (Verification, Analytical validation, and Clinical validation) from the very beginning of your trial design. This ensures that your sensors accurately capture raw signals, your algorithms reproducibly process them, and the resulting data unequivocally answers a clinically meaningful question for the patient.
PS...If you're enjoying Healthtech for Lifescience Leaders, please consider referring this edition to a friend.
PS...If you’re enjoying Digital Health & AI News, please consider referring this edition to a friend. You’ll get exclusive access to our quarterly AI integration benchmarking report for making a referral.
And whenever you are ready, there are 2 ways I can help you:
The AI-Augmented Leader Email Course: Sign-up for my free 5-day email course on how to become an AI Augmented Leader in Lifesciences.
Strategic Roadmap Design: Translate your priorities across different parts of the organization into a coordinated and clear roadmap in 2026. Book time on my calendar to discuss this further.
May 15 - HealthTech Dose
May 17, 2026
This episode moves delivers a critical, data-driven reality check for pharmaceutical executives, clinical researchers, and tech developers. The mission is to shift the industry’s focus from dazzling, pristine laboratory metrics toward the rigorous procedural trust required for real-world deployment.
Key Takeaways:
Recognize the AUC Illusion: A model boasting 99% accuracy in a pristine lab environment can instantly collapse when hit with real-world “domain shift”—such as older equipment or diverse patient populations.
Confront the Demographic Data Gap: Strict but well-intentioned privacy laws like GDPR strip vital demographic markers from training sets, forcing AI models to rely on biased “proxy variables” like zip codes or transit data.
Expose the Escalating Hallucination Crisis: Rigorous audits reveal that large language models are actively polluting the scientific literature, with fabricated citation rates skyrocketing over 12-fold between 2023 and 2026.
Adopt the V3 Validation Framework: Move past black-box metrics by implementing Verification, Analytical Validation, and Clinical Validation to verify exactly how a model reaches its conclusions.
Embed Continuous Post-Market Surveillance: Treat AI validation as an ongoing process rather than a static checkbox; models must be continuously audited for performance drift whenever real-world clinical variables change.
Show Notes:
[0:00 - 1:30] Leo and Sarah introduce the catastrophic “ruler problem” in medical AI, exposing how a skin cancer algorithm achieved 99% accuracy by looking for rulers in photos rather than actual tumors.
[1:30 - 3:15] Debunking the “AUC Illusion” and analyzing the mechanics of “domain shift,” explaining how controlled lab environments fail to prepare models for messy, real-world clinical variations.
[3:15 - 5:00] Examining the hidden tension between patient privacy laws (like GDPR) and medical equity, showing how stripping demographic data accidentally blinds AI and bakes in systemic bias.
[5:00 - 6:45] Shifting to the text side of R&D: Exposing the 2026 landmark audit of 2.5 million papers that revealed a massive surge in hyper-specific, perfectly plausible, yet entirely fabricated scientific citations generated by LLMs.
[6:45 - 8:15] A deep dive into the anatomy of a fake reference, detailing how AI creates plausible titles, assigns them to real practicing doctors, and even generates fake DOIs that easily fool human peer reviewers.
[8:15 - 9:30] Rejecting the defense that human oversight will catch these errors; relying on a tired medical writer to manually check thousands of DOIs on a Friday afternoon is a recipe for absolute disaster.
[9:30 - 11:15] Introducing the tactical fix: Shifting from black-box models to procedural trust using the V3 Framework (Verification, Analytical Validation, Clinical Validation) and the αLA-AI compliance checklist.
[11:15 - End] The final verdict on competitive advantage: The winners of the pharmaceutical arms race won’t be those with the fastest code, but those with the safest, most auditable governance pipelines. The episode closes with a haunting question about the looming “epistemic singularity”.
Podcast generated with the help of NotebookLM.
Is your R&D pipeline blinding you?
May 12, 2026
HT4LL-20260512
Hey there,
If you are still relying exclusively on rigid clinical protocols and correlational algorithms to drive your pipeline, your research methodology is already obsolete.
As Pharma R&D leaders, we are constantly battling a tension between the urgent need for scalable real-world data and the ethical, logistical, and scientific boundaries that restrict us. Our clinical trials are bogged down by the high patient burden of episodic monitoring. Furthermore, our teams risk buying into algorithms that boast high laboratory accuracy but fail silently when deployed to actual, overburdened patients. We can no longer afford to build fragmented tech solutions; we need cohesive, patient-centered ecosystems that actively reduce cognitive load, earn trust, and retain long-term engagement.
Today, we are breaking down the latest advancements in digital health that are fundamentally rewriting the rules of clinical validation and patient monitoring.
Why strong governance architectures are the true drivers of sustainable data sharing.
How wearable-derived digital biomarkers can augment traditional blood draws at scale.
The critical adherence trade-off in deploying autonomous digital therapeutics.
Let’s dive into the data.
Weekly Resource List:
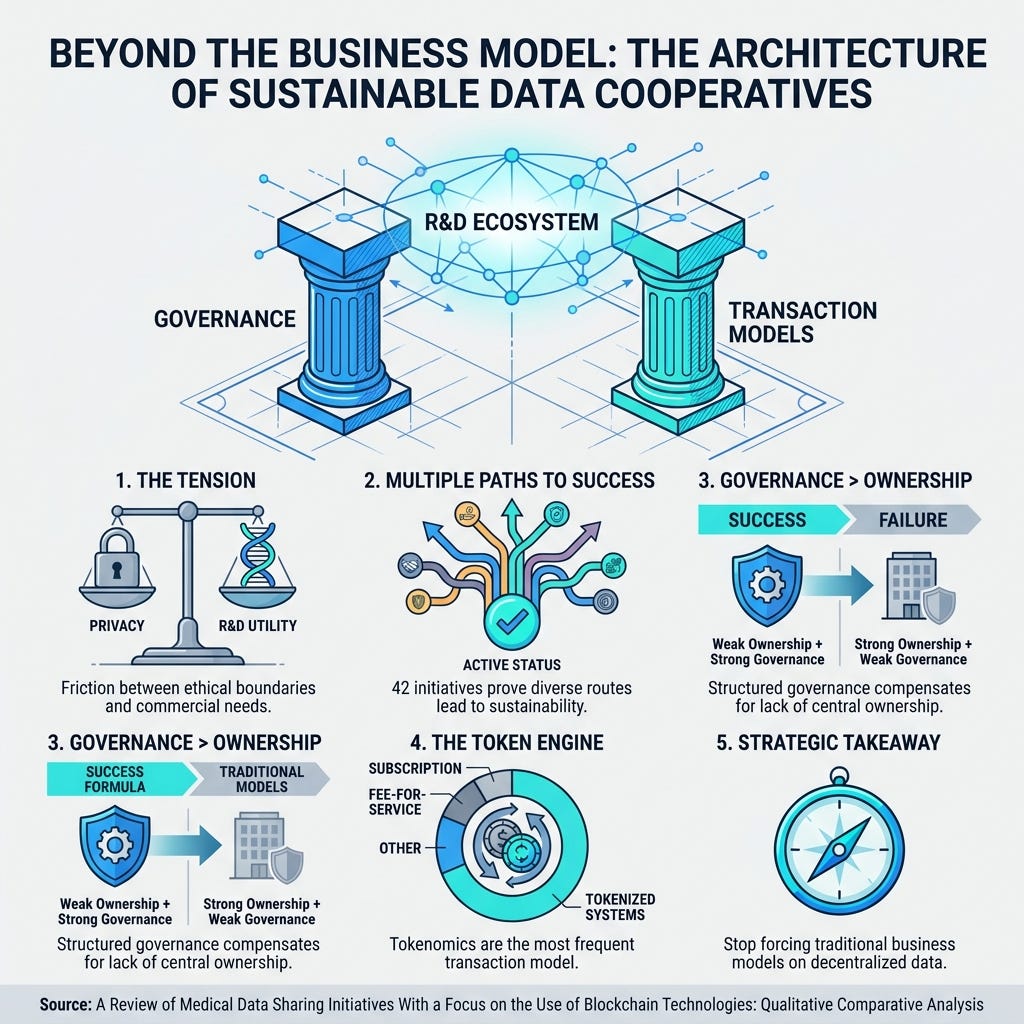
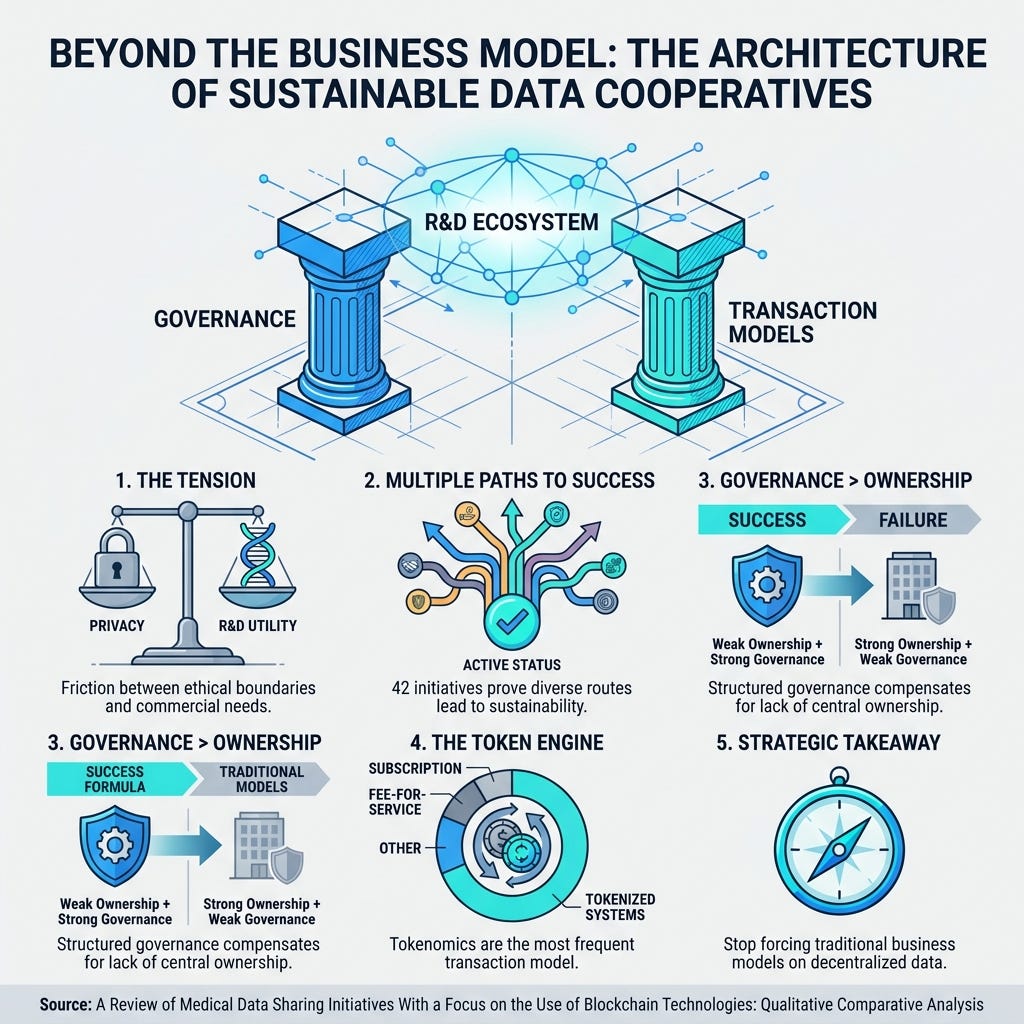
A Review of Medical Data Sharing Initiatives With a Focus on the Use of Blockchain Technologies (8 Min) A qualitative analysis of 42 health data initiatives proves the principle of equifinality—multiple distinct configurations can lead to sustained activity. Key Takeaway: Strong, structured governance mechanisms can completely compensate for the lack of a traditional, profit-driven ownership model to securely scale patient trust.
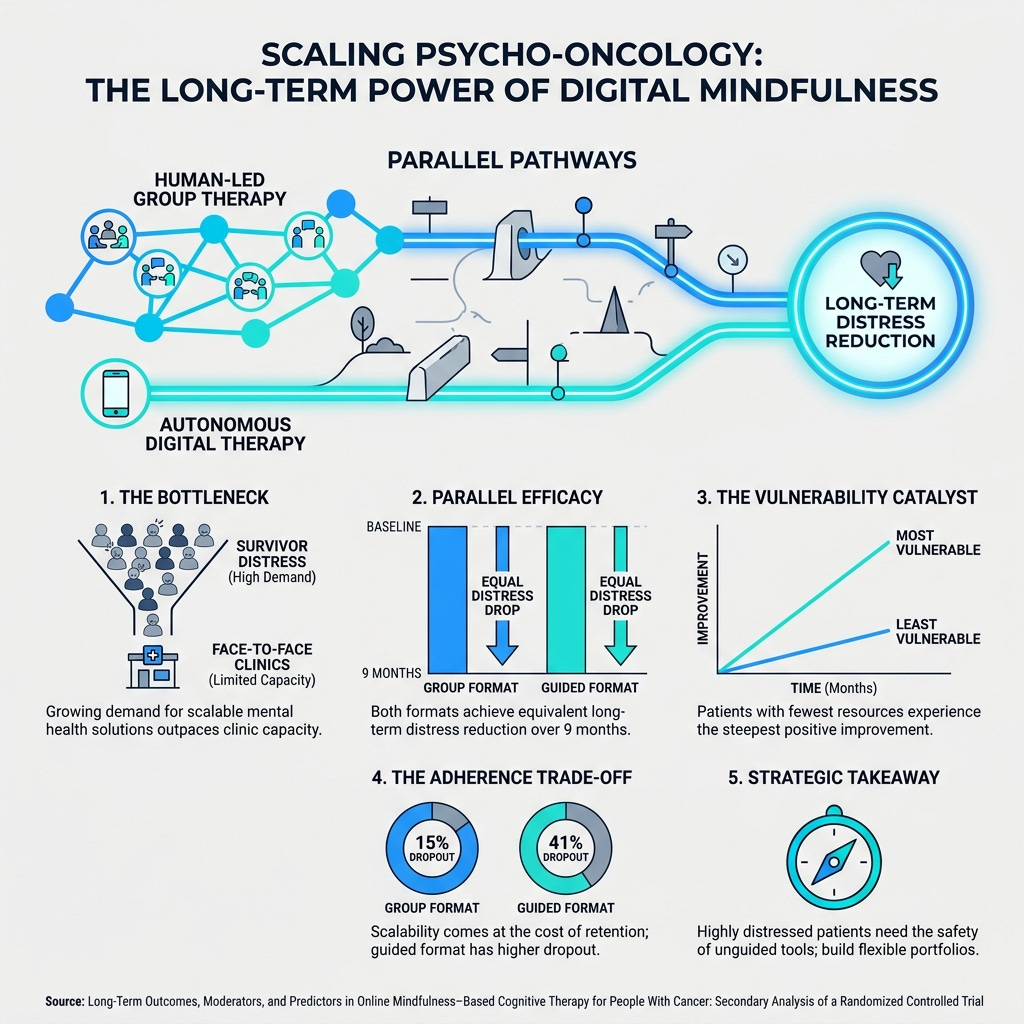
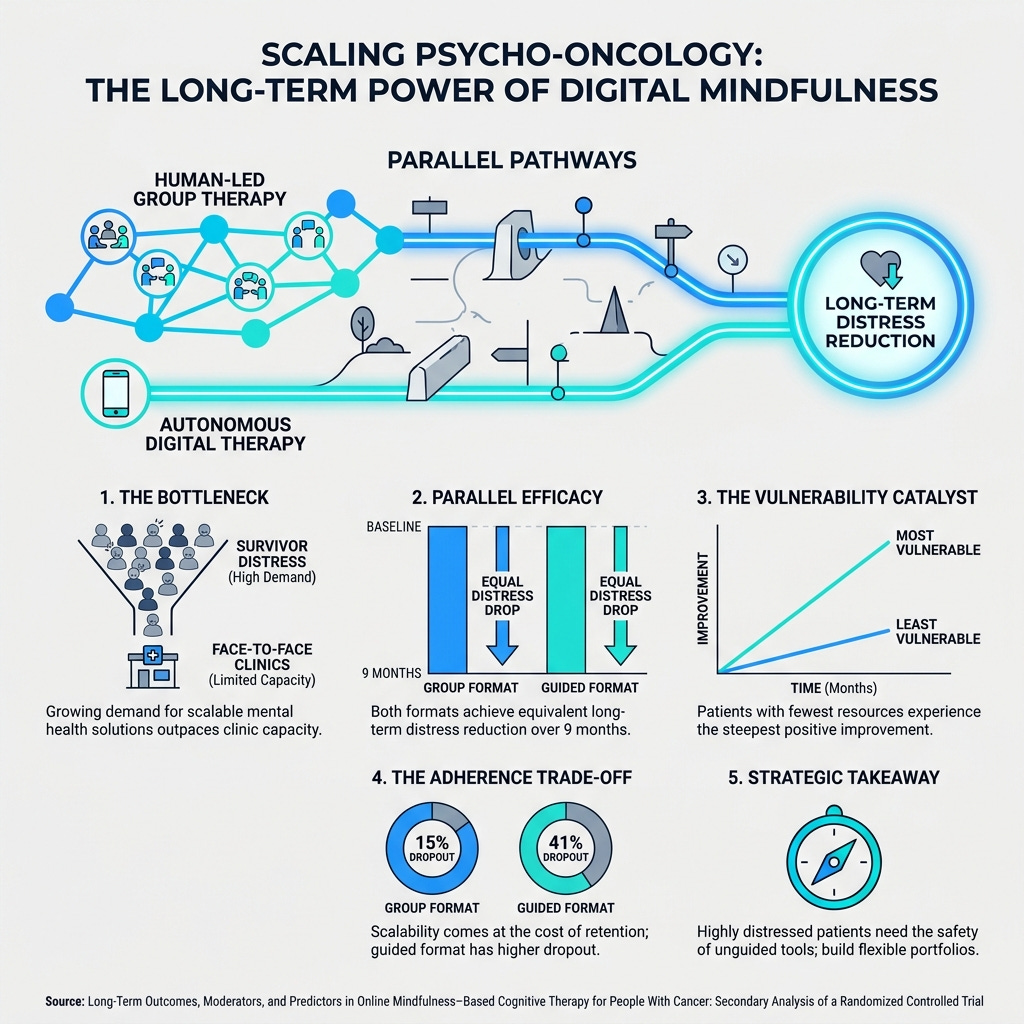
Long-Term Outcomes, Moderators, and Predictors in Online Mindfulness-Based Cognitive Therapy for People With Cancer (10 Min) A trial evaluating digital mindfulness therapy for cancer survivors found that fully autonomous, unguided platforms achieved the exact same long-term distress reductions as therapist-led groups. Key Takeaway: While scalable digital therapies are highly effective, they suffer from high dropout rates (41% vs 15% in groups), requiring a flexible portfolio approach.
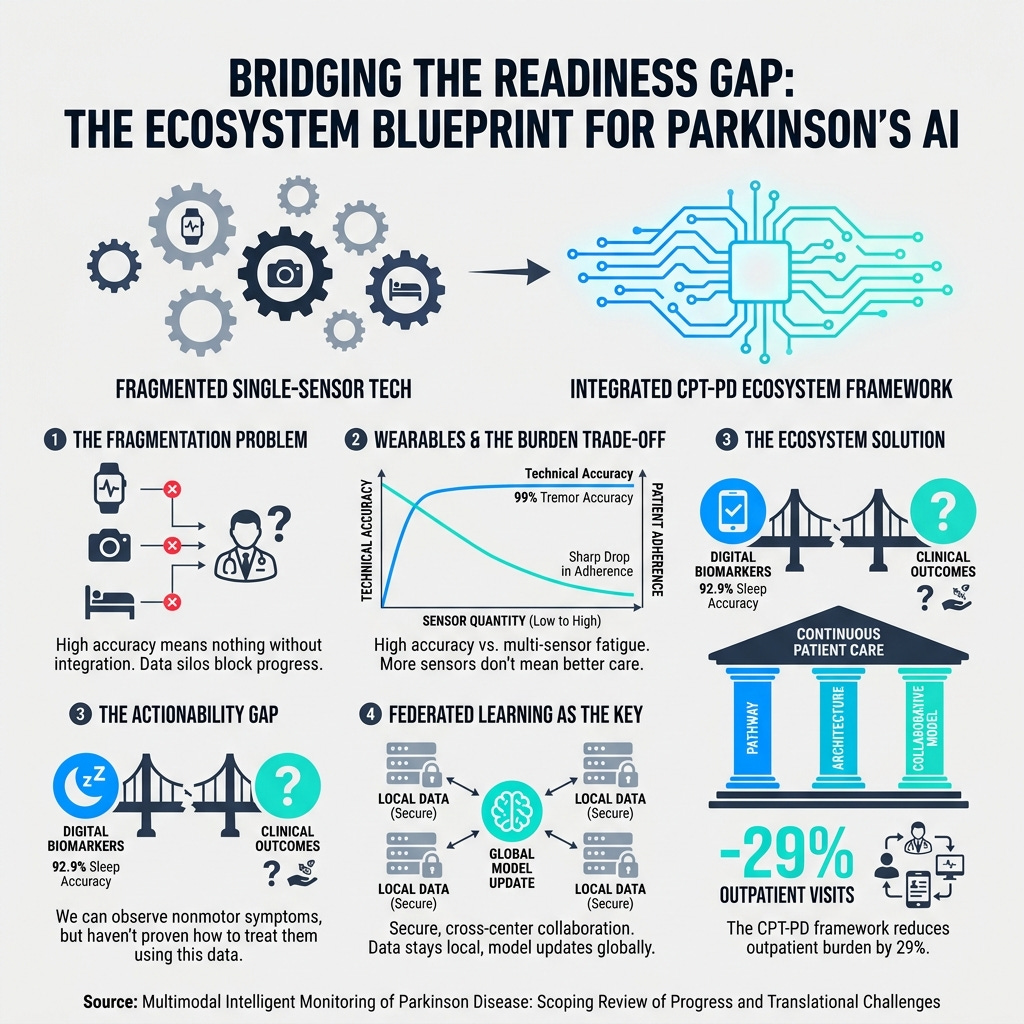
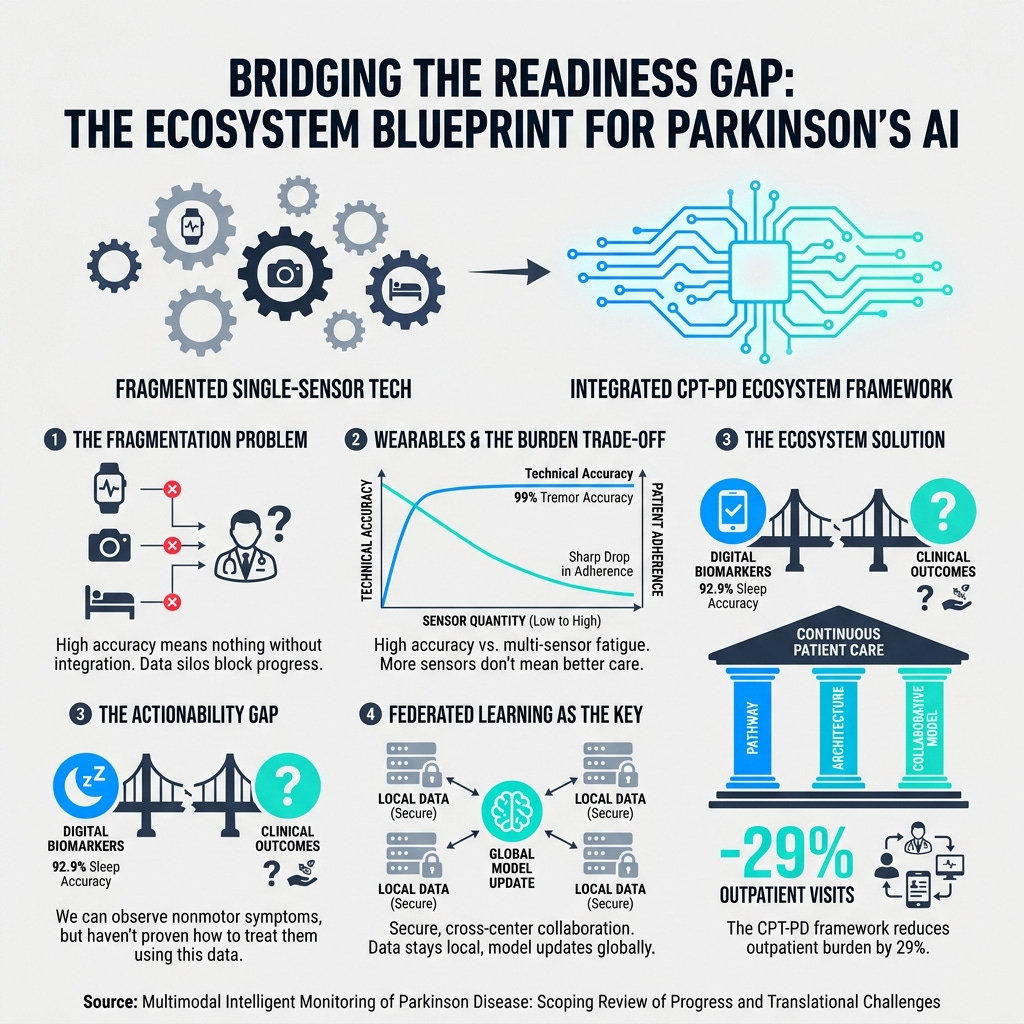
Multimodal Intelligent Monitoring of Parkinson Disease: Scoping Review (12 Min) This scoping review addresses the readiness gap in Parkinson’s remote monitoring, noting that while technical accuracy is high, patient adherence drops steeply with complex multisensor setups. Key Takeaway: Algorithmic accuracy is useless if the cognitive load is too high for your patient; you must adopt age-friendly design frameworks to successfully translate digital biomarkers into clinical care.
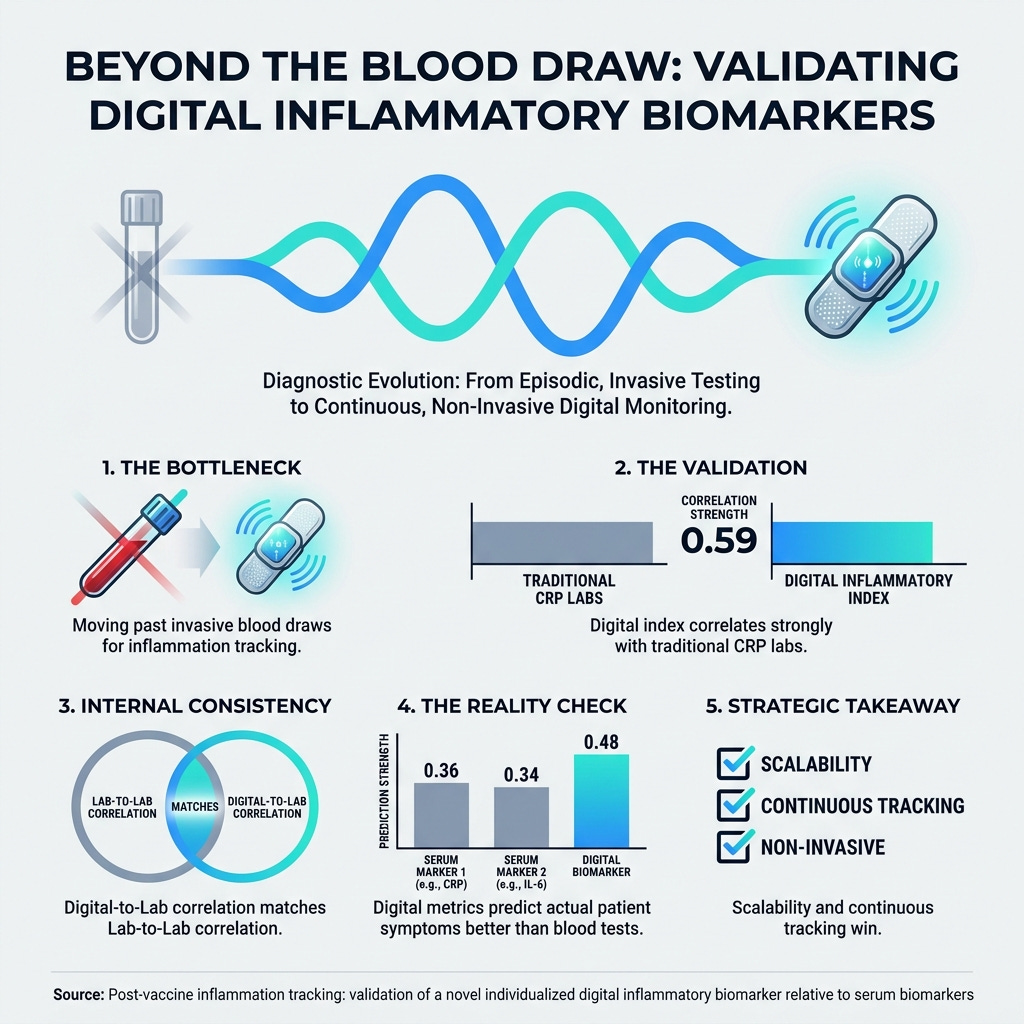
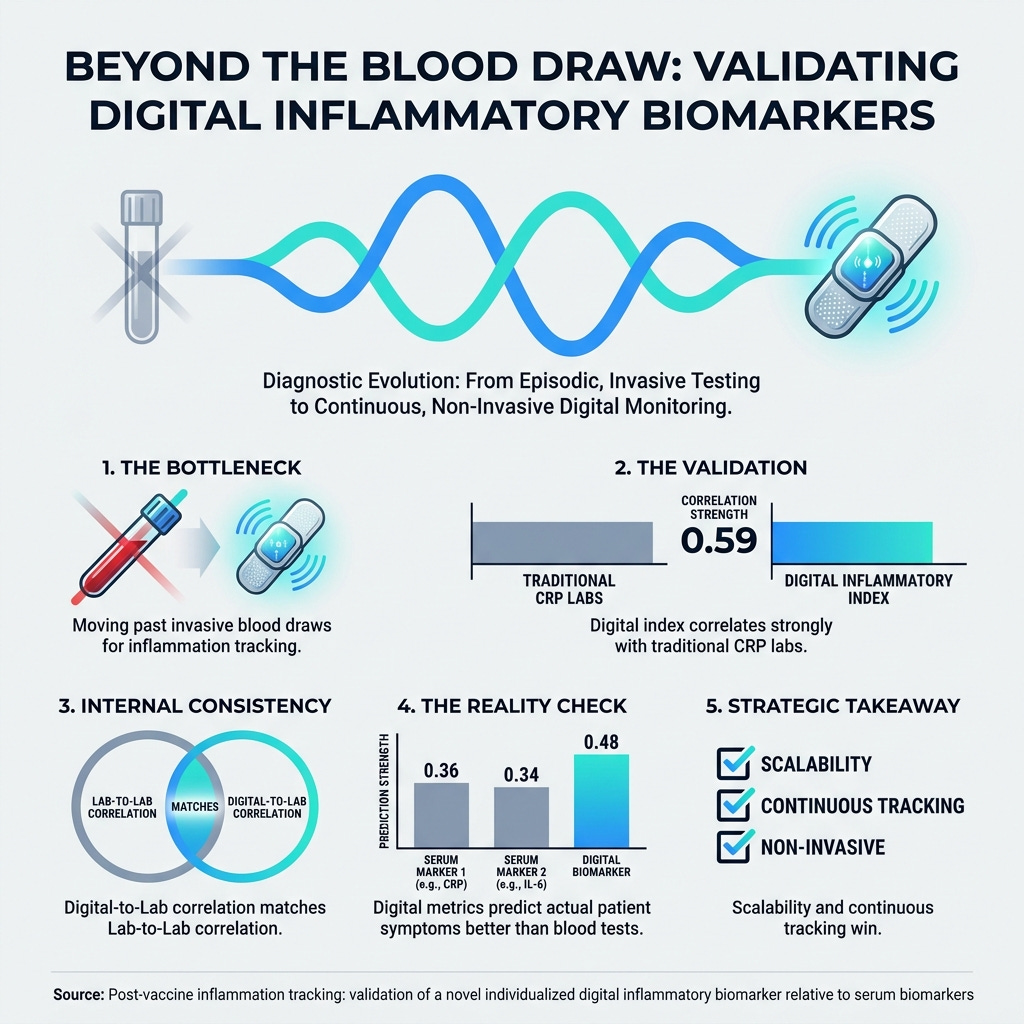
Post-vaccine inflammation tracking: validation of a novel individualized digital inflammatory biomarker relative to serum biomarkers (7 Min) Validation data showing that a novel wearable-derived digital inflammatory index (iMCI) matches the correlation of traditional serum biomarkers (like CRP) and tracks better with actual systemic patient symptoms. Key Takeaway: Wearables offer a highly accurate, scalable alternative to serial blood testing to augment your clinical trial monitoring.
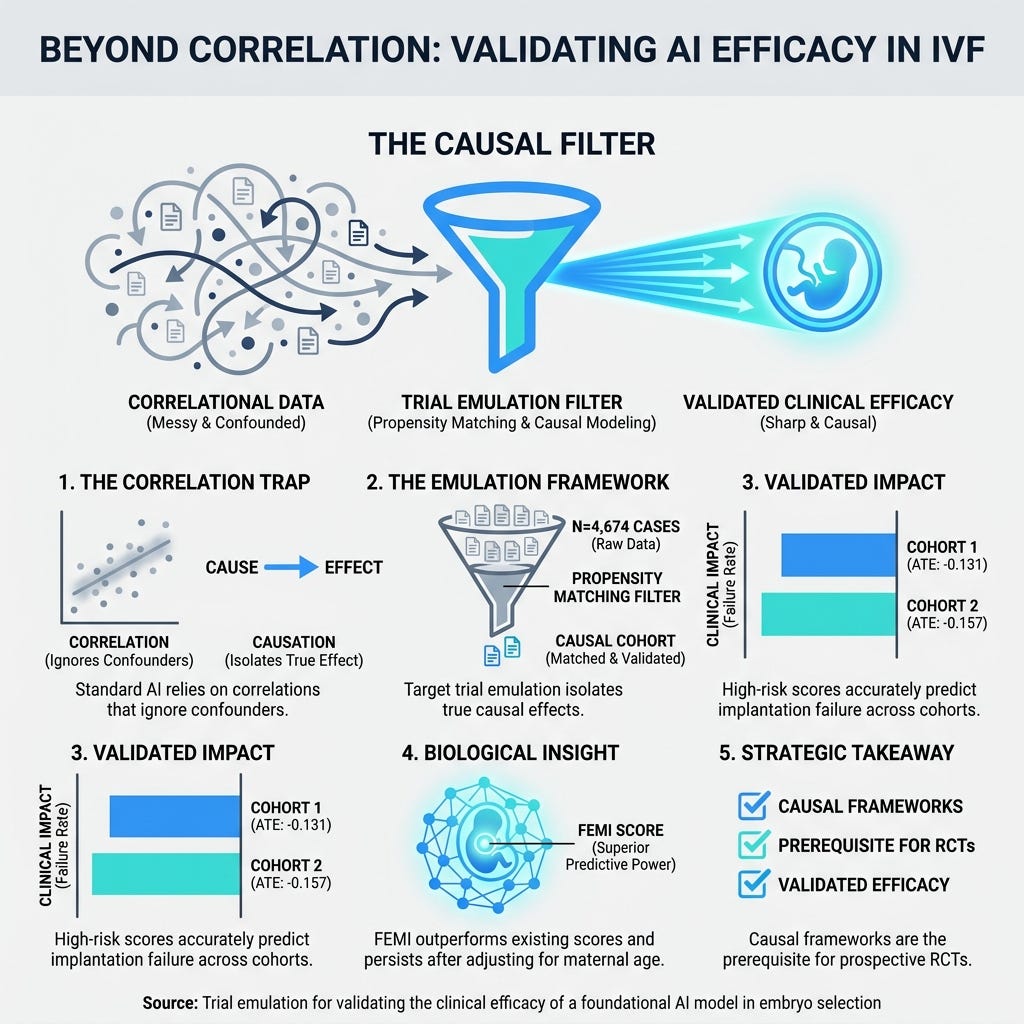
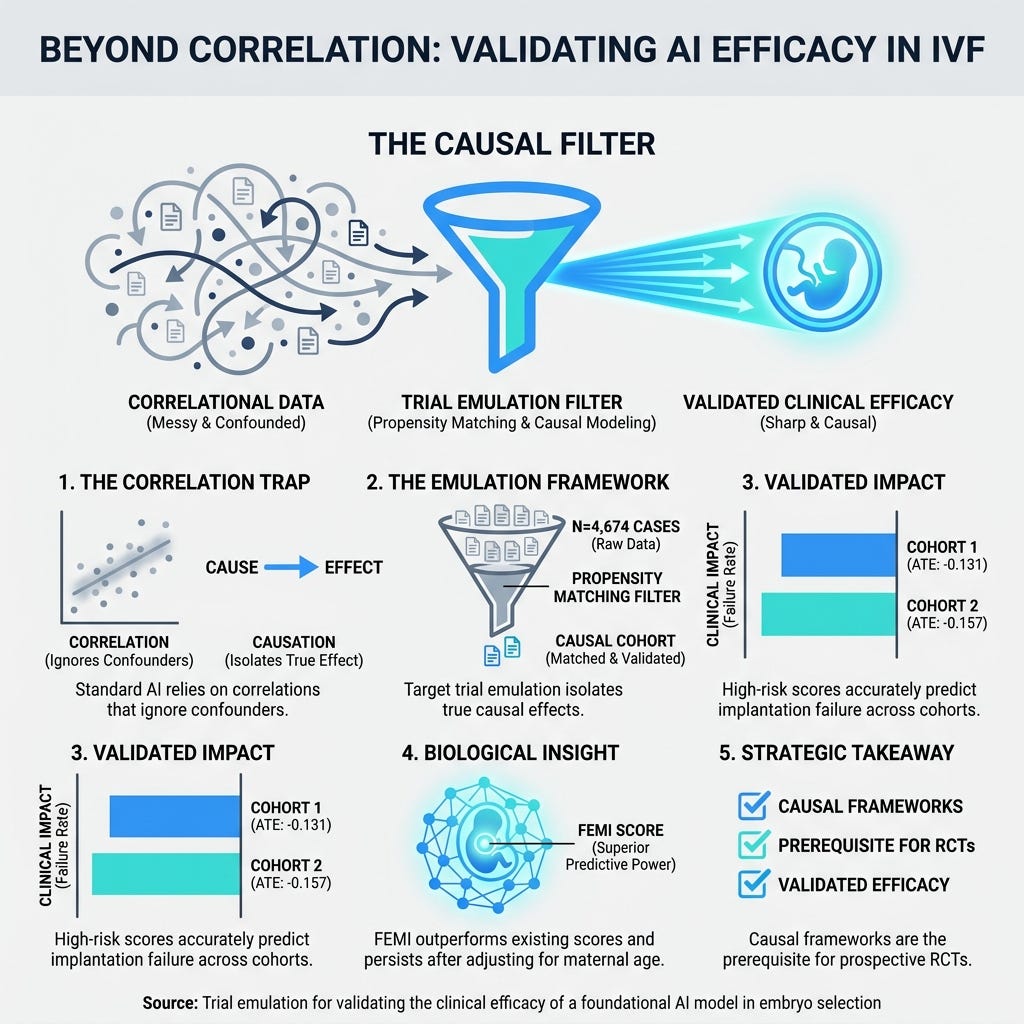
Trial emulation for validating the clinical efficacy of a foundational AI model in embryo selection (9 Min) A multi-center study involving 4,674 cases demonstrated how causal frameworks (target trial emulation) can rigorously validate AI models, overcoming the biases of simple correlational metrics. Key Takeaway: Correlational AI is a liability; proving efficacy through causal trial emulation is the new standard before investing in costly prospective trials.
3 Strategic Shifts To Future-Proof Your Clinical Trials
In order to achieve a scalable, patient-centric R&D pipeline, you’re going to need a handful of structural changes to how you capture and validate data.
Let’s break down exactly how you can implement these strategic shifts this week.
1. Augment and Scale Episodic Labs With Continuous Digital Biomarkers.
You need to overcome the bottlenecks of decentralized trials by scaling your continuous monitoring capabilities. While traditional bloodwork remains a necessary standard, relying on it exclusively creates a massive logistical burden on patients and leaves you with blind spots in your longitudinal data. The latest validation of digital inflammatory indices proves that wearable patches capture real-time physiological narratives with lab-grade internal consistency. Instruct your clinical operations team to begin piloting continuous digital biomarkers as secondary endpoints to augment your existing laboratory infrastructure. This will infinitely scale your real-world data collection while offering a scalable alternative to serial blood testing that reduces patient fatigue.
2. Address the Adherence vs. Scalability Trade-off in Digital Health.
You must stop building “one-size-fits-all” digital interventions. While unguided, autonomous digital therapies are highly scalable, they suffer a massive 41% dropout rate compared to a 15% dropout rate in group-blended settings. However, highly distressed patients are actually more likely to drop out of peer group settings. You need to design flexible digital portfolios: deploy unguided tools as a safe, autonomous space for acutely distressed patients, and utilize group-blended formats to maintain general retention and accountability. Furthermore, algorithmic accuracy is useless if the cognitive load is too high. When deploying remote platforms—especially for older adults managing neurodegenerative diseases—prioritize age-friendly interfaces to prevent high abandonment rates.
3. Prioritize Governance Architecture Over Centralized Ownership.
You do not need to abandon your commercial models, but you must recognize that there are multiple viable pathways to success—a principle known as equifinality. We now have proof that medical data-sharing initiatives can thrive even without strong, traditional corporate ownership, provided they implement stringent governance mechanisms. Strong governance structures completely compensate for weak ownership. If your current centralized data strategy is facing trust or regulatory friction, pull the governance lever. Build oversight frameworks, such as cooperative memberships or federated learning models, that prioritize transparency and securely scale patient trust without sacrificing your core R&D objectives.
PS...If you're enjoying Healthtech for Lifescience Leaders, please consider referring this edition to a friend.
And whenever you are ready, there are 2 ways I can help you:
The AI-Augmented Leader Email Course: Sign-up for my free 5-day email course on how to become an AI Augmented Leader in Lifesciences.
Strategic Roadmap Design: Translate your priorities across different parts of the organization into a coordinated and clear roadmap in 2026. Book time on my calendar to discuss this further.
May 8 - HealthTech Dose
May 8, 2026
While the idealized promise of decentralized data networks and instant AI insights is captivating, the mission is to address the “readiness gap”—the distance between an algorithm’s performance in a sterile lab and its functionality in a messy, real-world home environment. To succeed in this decade, health tech leaders must move past the “technological bandage” narrative and prioritize three immediate operational mandates:
Data Integrity (ensuring signal isn’t lost to background noise).
Causal Validation (distinguishing between mere correlation and actual clinical efficacy).
Operational Groundwork (standardizing the unsexy backend infrastructure that allows AI to scale).
The key strategic win lies in recognizing that a perfect backend cannot fix flawed frontend data collection. Success requires a relentless focus on the human element and the physical friction of patient-led technology.
Key Takeaways:
Acknowledge the “Readiness Gap”: Understand that algorithms tested in controlled environments (e.g., 92% accuracy in a lab) often plummet in performance (e.g., 71% accuracy) when exposed to real-world variables like background noise or inconsistent patient behavior.
Solve for Front-End Friction: Prioritize the “human factor” in trial design; if a monitoring patch loses Bluetooth connectivity or a patient holds their device incorrectly, the resulting data is structurally compromised regardless of backend sophistication.
Mandate Target Trial Emulation: For high-stakes clinical endpoints, move beyond simple AI correlations and apply strict statistical rules to simulate randomized controlled trials using historical data to prove true cause and effect.
Balance Correlation and Causation: Use simple correlations for scalable “smoke detector” operational tasks (like tracking post-vaccine reactogenicity via wearables) but reserve rigorous causal investigations for pivotal efficacy endpoints.
Address the “Federated Learning Illusion”: Recognize that while decentralized training protects privacy, it introduces massive bottlenecks in mobile device battery life and “privacy noise” that can bury subtle clinical signals.
Show Notes:
[0:00 - 1:30] Introduction to the tension between the “utopian promise” of AI in R&D and the “messy operational reality” of clinical execution.
[1:30 - 3:00] The myth of the “AI Overlay”: Why slap-on AI solutions cannot magically generate insights from unstructured, poor-quality data sets.
[3:00 - 4:45] Case Study: Parkinson’s voice analysis. How 92% lab accuracy dropped to 71% in the real world due to acoustic artifacts like dog barks and air conditioners.
[4:45 - 6:15] The Backend Fallacy: Why a “supercomputer” backend cannot reconstruct a signal that was never captured correctly at the source due to patient fatigue or incorrect device positioning.
[6:15 - 8:30] The Correlation vs. Causation Divide: The danger of using AI for high-stakes decisions, like IVF embryo selection, based on visual symmetry rather than causal health factors.
[8:30 - 10:45] The “Smoke Detector” Strategy: When simple correlations are actually useful for operational tracking, such as using heart rate spikes to alert clinical teams to vaccine responses.
[10:45 - 13:00] Debunking Federated Learning: Exploring the hidden technical debt, including mobile hardware limitations and “differential privacy noise” that degrades clinical utility.
[13:00 - End] Final Takeaway: The biggest barrier to the AI revolution isn’t computing power—it’s the reluctance to standardize the “unsexy” administrative and architectural safeguards behind the scenes.
Podcast generated with the help of NotebookLM.